





I. Introduction
Levator ani syndrome (LAS) manifests as functional pain lasting over 30 minutes in the regions of the rectum, sacrum, and coccyx, presenting as a mixed mode of pain, pressure, and discomfort1. LAS is characterized by recurrent or chronic rectal pain, primarily triggered by prolonged sitting or defecation2. The levator ani muscles, composed of the puborectalis, pubococcygeus, and iliococcygeus muscles, provide support to the viscera in the pelvic cavity3. LAS is recognized to result from a painful spasm of the levator ani muscles4, however its etiology remains unknown as no detectable organic pathology has been identified4. Notably, psychosocial distress, such as depression and anxiety, significantly influences LAS in many individuals5. Given the increased vulnerability of women to psychological distress6, LAS is more prevalent in women, particularly those aged 30-60 years7. According to a national survey in the USA, the prevalence of LAS was 6.6%, with a 1.4-fold higher occurrence in women (7.4%) compared to men (5.4%)8.
Various therapeutic approaches, including biofeedback, electrogalvanic stimulations, and digital massage, have been employed to alleviate rectal discomfort. However, the efficacy of these methods is limited in managing LAS9. While some advocate transperineal botox injections as a relief method for levator spasm, caution is warranted due to potential contraindications, such as hypersensitivity to botox and concomitant neuromuscular disorders10. To date, no singular treatment has proven universally successful for LAS patients, especially those experiencing severe pain unresponsive to the aforementioned interventions.
This study aims to report a case of a chronically refractory LAS patient whose condition significantly improved with traditional Korean medicine (TKM) -based treatments.
II. Report of the case
1. Characteristics of the Patient and Medical History
A 47-year-old man sought medical attention at a Korean medicine hospital due to chronic anorectal pain. The pain, ranging from moderate to sometimes severe, typically manifested during morning defecation and persisted until noon. The severity of the pain diminished when lying down but exacerbated during prolonged periods of standing or sitting. As a consequence of the anal pain, the patient experienced fatigue easily and a reduced work efficacy. Despite visiting multiple hospitals, no specific medical abnormalities were detected through examinations, and there was no improvement with medications.
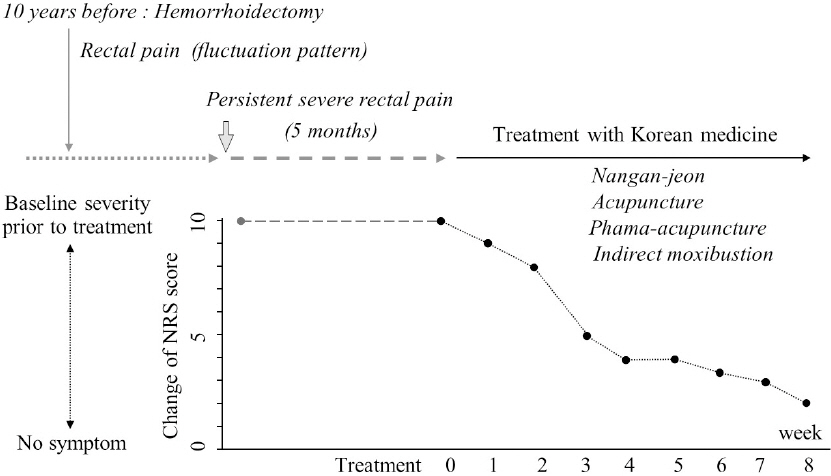
The onset of his anorectal pain occurred 10 years ago, with no specific triggering episode except for a past hemorrhoidectomy. The pain persisted for a decade, with sporadic disappearances lasting approximately 2 years. Over the last 5 months, there has been a worsening of both the severity of pain and its duration, despite no changes in triggering factors. The patient has a body mass index (BMI) of 23, abstains from alcohol and smoking, and exhibits a meticulous nature. Additionally, he faces stressors in his role as a university professor outside of Korea. This case study had been approved by the Institutional Review Board for Human Research of Daejeon University Daejeon Hospital (#: DJDSKH -24-E-05-1).
2. Diagnosis
Given the absence of any abnormalities in previous hospital examinations and the presence of anorectal pain, the patient was diagnosed with LAS. Examination of the tongue revealed a mild pinkish-white color, and the pulsation was weak and rapid. The patient exhibited slight tenderness and stiffness in the low abdominal area, alleviated by warm application. The author identified the pattern as “liver-kidney deficiency cold (肝腎虛寒)”.
3. Treatments and Course of Symptoms
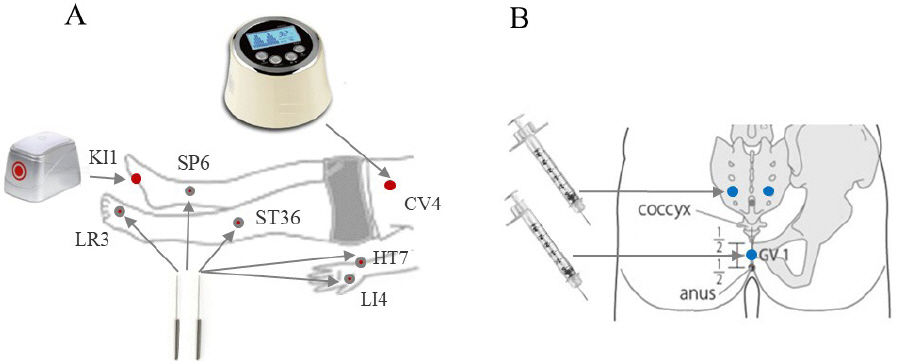
Based on the pattern differentiation, the herbal drug Nangan-jeon (暖肝煎) was prescribed with modifications and administered orally twice daily, as detailed in Table 1. In addition to herbal treatment, the patient underwent acupuncture weekly, focusing mainly on bilateral HT7, ST36, SP6, and LR3 acupoints for 20 minutes (using 0.25×30 needles from DongBang Co., Seoul) Indirect moxibustion (using electric moxibustion from TechnoSience Co., Seoul) was applied at both CV4 and KI1 for 25 min, and 2 mL of Aconitum Ciliare Decaisne pharmacopuncture (from GiRin extramural herbal dispensaries, WonJu) was administered at GV1 and BL33 acupoints (Fig. 1). After one week of treatment, self-reported numerical rating scale (NRS) scores indicated a 9-point in anorectal pain (with 10 representing baseline pain at the initial visit and 0 indicating no pain). By the end of the third week, the pain had decreased by NRS 5. After 8 weeks of treatment, the patient reported a NRS 2 of the anorectal pain, expressing satisfaction. Subsequently, the patient returned to his home country (Fig. 2).
Table 1
Composition of Modified Nangan-jeon
| Scientific name | Herbal name | Chinese name | Dose* |
|---|---|---|---|
| Lycium chinense Miller | Lycii Fructus | 枸杞子 | 24.0 g |
| Angelica gigas Nakai | Angelicae Gigantis Radix | 當 歸 | 16.0 g |
| Poria cocos Wolf | Poria Sclerotium | 白茯苓 | 16.0 g |
| Foeniculum vulgare Miller | Foeniculi Fructus | 小茴香 | 16.0 g |
| Lindera strichnifolia Fernandez-Villar | Linderae Radix | 烏 藥 | 16.0 g |
| Cinnamomum cassia Presl | Cinnamomi Cortex | 肉 桂 | 8.0 g |
| Saussurea lappa Clarke | Saussureae Radix | 木 香 | 4.0 g |
| Artemisiae Argyi | Artemisiae Agyi Folium | 艾 葉 | 16.0 g |
| Leonurus japonicus Houtt. | Leonuri Herba | 益母草 | 16.0 g |
| Cyperus rotundus L. | Cyperi Rhizoma | 香附子 | 12.0 g |
| Rubus coreanus Miq. | Rubus Coreanus | 覆盆子 | 12.0 g |
| Alpinia oxyphylla Miq. | Alpinia oxyphylllae Fructus | 益智仁 | 12.0 g |
III. Discussion and Conclusion
The current study describes a male case of chronic and refractory LAS. The LAS symptoms began without any apparent cause, except for a hemorrhoidectomy performed 10 years ago. While there is limited data available on LAS, chronic anal pain can seldom occur following anorectal surgeries, including hemorrhoidectomy11. The patient in this case observed that his LAS commenced at some point after the hemorrhoidectomy, rather than immediately post-surgery. Due to the initially mild nature of the pain, the patient cannot recall precisely when it began, but over the course of 10 years, it progressively worsened.
Although not specific for LAS, there are several therapeutics for anorectal pain including biofeedback or digital massage. The LAS symptom of this case patient had not been improved by any treatments in Wester clinics before. The patient had received acupuncture treatments in US due to living in US as an immigrant, but it was not effective for his pain. He read my case report of a severe woman LAS after hemorrhoidectomy, which was improved by traditional Korean medicine12. The anorectal pain of this present patient had been reduced rapidly from just after 1 weeks, and reached to the satisfaction level finishing treatments after 8 weeks (Fig. 2). These choices of treatments were decided based on the diagnosis by Korean medicine system.
While not specific to LAS, various therapies exist for anorectal pain, such as biofeedback or digital massage. In the case of this patient, LAS symptoms had not responded to any treatments in Western clinics previously. Despite receiving acupuncture treatments in the U.S. as an immigrant, the patient found no relief from his pain. After coming across my case report detailing the successful treatment of severe LAS in a woman following hemorrhoidectomy12, the present patient decided to explore this approach. Remarkably, the anorectal pain of the current patient significantly diminished just one week into the treatment, ultimately reaching a satisfactory level by the conclusion of the 8-week treatment period (Fig. 2). These treatment choices were made based on the diagnosis provided by the Korean medicine system.
In the context of treatments derived from Korean medicine, the patient received acupuncture, pharmacopuncture, indirect moxibustion, and herbal decoction. The selection of acupoints aimed at modulating the psychological stress response (HT7), adjusting the threshold of visceral sensation (ST36 and SP6), and enhancing gastrointestinal (GI) motility (both LR3 and LI4) (Fig. 1A). Numerous studies have reported results supporting these applications, including the potential anti-psychological stress effects of HT713,14, as well as the improvement of functional rectal pain or modulation of gut-brain interaction through acupuncture at ST36 and SP615-17. LR3 and LI4, collectively known as Siguan meaning ‘four gates,’ are specifically applied to enhance GI motility, supported by various clinical evidences18,19. Clinical trials have demonstrated the effectiveness of acupuncture in reducing rectal pain after hemorrhoidectomy20.
Furthermore, the patient was treated with pharmacopuncture (administered at GV1 and BL33 acupoints) composed of Aconitum Ciliare Decaisne, a representative herbal plant known for its anti-pain pharmacological activity21. The patient also received a modified Nangan-jeon (暖肝煎) (Table 1). This prescription was selected based on the pattern identification of “liver-kidney deficiency cold (肝腎虛寒)”, guided by the characteristics of a tender and cold lower abdomen, a pinkish-white tongue color, and weak-rapid pulsation. Described initially in the Gyeongakjeonseo (景岳全書), this herbal formula addresses the pathological condition of ‘cold symptoms of the liver- and kidney-Yin’22. Numerous clinical studies have reported the efficacy of Nangan-jeon (暖肝煎) in various applications, such as refractory abdominal pain in the elderly23 and in patients with Lambert–Eaton myasthenic syndrome24. For this particular patient case, several herbs, including Leonuri Herba and Cyperi Rhizoma, were added to the formula. These additions serve to warm the intestine and provide relief from pain25,26.
LAS is recognized as a spasm affecting the Levator ani muscles, including the puborectalis, pubococcygeus, and iliococcygeus muscles. However, a particular study noted a tendency toward hyper-contractile external anal sphincter rather than spasm in LAS27. Therapeutic options for LAS encompass various approaches, such as biofeedback therapy, digital massage, sitz baths, diathermy, and muscle relaxants28. Nevertheless, some cases remain unresponsive to these treatments, resulting in persistent impairment of daily life. Notably, there are only a few academic reports on the treatment of LAS using TKM, including acupuncture in the United States29.
In summary, this case study underscores the clinical potential of TKM-based treatments for refractory LAS. As further clinical applications unfold, TKM could emerge as a common therapeutic option for LAS in the future.


