4도 욕창 환자에 대한 가미십전대보탕 투여 및 침치료와 습윤드레싱의 병행 효과 : 치험 1례
Abstract
Introduction:
Pressure ulcers, often found in patients with mobility issues, particularly elderly patients, are increasing in prevalence. Their treatment is complex, with recovery more challenging in advanced stages, and certain factors can delay healing.
Case Presentation:
An 87-year-old male developed a grade IV pressure ulcer on his left greater trochanter following lumbar fractures and subsequent percutaneous vertebroplasty in 2021. Despite potential surgical recommendations, his treatment consisted of daily wet dressings, acupuncture from July 2021 to February 2022, and Gami-sipjeondaebo-tang beginning August 2021. The ulcer, initially measuring 6 cm×6 cm and showing a red wound without necrosis, healed completely and showed no signs of recurrence as of August 2023.
Conclusion:
A grade IV pressure ulcer was effectively treated using wet dressing, acupuncture, and Gami-sipjeondaebo-tang, demonstrating no recurrence over a 1.5-year period.
Keywords: acupuncture, Gami-sipjeondaebo-tang, pressure ulcer, wet dressing
I. 서 론
욕창은 지속적이고 일정한 압력을 받는 부위의 피부, 피하지방, 근육 부위에 혈액 순환이 장애를 받아 허혈 상태가 되면서 이로 인해 궤양이 발생하는 것이다 1. 따라서, 욕창은 거동이 어려운 뇌혈관질환 환자, 척수손상 환자, 고령에서 발생 빈도가 높다 2. 국내 욕창 환자 수는 2016년 21,670명, 2017년 23,554명, 2018년 25,562명으로 점점 증가하고 있으며, 이 중 70~79세가 27.7%, 80세 이상이 54.5%로 상당수를 차지하고 있다 3. 특히, 척수 손상 환자의 욕창 발생률과 관련하여 여러 연구 결과에 따르면 척추 손상 후 1년 안에 약 15%, 20년 안에 약 26% 정도의 환자들이 크고 작은 욕창을 경험하고 있다 4. 욕창의 치료는 National Pressure Ulcer Advisory Panel(NPUAP) 분류에 따라 비수술적 치료와 수술적 치료 두 가지로 나눌 수 있다 5. 수술적 치료는 일반적으로 3도 이상의 욕창에 권장된다 5. 보존적 치료를 할 경우 완치까지 걸리는 기간은 1도 욕창은 1주, 2도 욕창은 2주에서 한 달, 3도 욕창은 4달에서 1년 정도로 알려져 있으며, 4도 욕창은 완화는 가능하나 완치는 어려운 것으로 본다 5. 만약 욕창 환자가 고령, 당뇨병, 고혈압, 대변실금, 저알부민혈증, 말초혈액순환의 장애 등이 있을 경우 완치까지의 기간은 더 오래 걸리게 된다 6. 본 증례의 대상자는 고령이며, 20년 이상 당뇨병과 고혈압을 가지고 있었고, 압박골절로 인한 척수손상 후 대변실금이 발생하였으며, 심혈관 문제로 인한 하지 부종 및 저림을 호소하는 등 말초혈액순환의 장애가 의심되는 상태였다. 그럼에도 불구하고 7개월 동안 시행된 한의치료 및 습윤드레싱 병행 요법에 의해 완치되었고, 이후 1년 6개월 동안의 추적관찰기간 동안 재발이 없었다.
본 증례 이외에도 한의치료를 통해 3도 혹은 4도 욕창을 치료했다는 증례들은 꾸준히 보고되고 있다 5,7-10. 하지만 이들 중 대부분의 증례들은 완치가 아닌 유의미한 호전을 보인 것을 보고하고 있으며, 본 증례처럼 장기간 추적관찰하여 재발여부까지 확인한 연구는 없었다. 이에 본 연구진은 이번 증례가 특별한 의의가 있는 것으로 판단하고 상세히 보고하고자 한다.
II. 증 례
본 증례는 CARE guidelines을 준수하였으며, ⃝⃝대학교 ⃝⃝한방병원 임상시험심사위원회 심의를 통과(WKIRB 2023-14)하였다.
1. 성별/나이 : 남(male) / 87세
2. 진단명 : 욕창궤양 4단계(Pressure Ulcer NPUAP Grade IV)
3. 진단일 : 2021년 04월 22일
4. 주 소 : 좌측 대전자(Left greater trochanter) 욕창
5. 현병력
2021년 01월 및 03월경 발생한 요추 압박골절로 척추성형술 시행 후 대소변장애 및 보행장애가 발생하였으며, 이로 인해 장기간 와상하게 되었다. 그러던 중 좌측 대전자의 욕창 발생하였고, 2021년 04월 22일 로컬병원에서 NPUAP 11( Supplementary Material 1) 분류상 욕창 Grade IV를 진단받고, 동병원 일반외과에서 욕창 부위의 변연제거술(debridement)을 통해 괴사 조직을 제거하였다. 이후 ⃝⃝대학교병원 성형외과 진료받았으며, 드레싱을 하며 경과관찰하고, 호전이 없을 시 수술이 필요하다는 소견을 들었다. 적극적인 치료 위해 2021년 07월 08일 본원으로 입원하였다. 6. 과거력
고혈압(20년 이상)과 당뇨병(20년 이상)을 가지고 있으며, 만성적인 하지 부종 및 감각 저하를 호소하여 말초혈액순환의 장애가 의심되었다. 또한, 2013년 관상동맥 협착 진단 및 경피적 관상동맥중재술을 받은 바 있다. 과거력과 관련하여 복용 중인 약물은 Table 1에 기술하였다.
Table 1
List of Drugs the Patient Was Taking
|
Brand names |
Dosage |
|
Dilatrend Tab. 12.5 mg |
0.5 Tab # 1 QD |
|
Telmican Tab. 40 mg |
1 Tab # 1 QD |
|
Neomaryl Tab. 1 mg |
0.5 Tab # 1 QD |
|
Rosulord Tab. 20 mg |
1 Tab # 1 QD |
|
Platless Tab. |
1 Tab # 1 QD |
|
Synerjet Tab. |
3 Tab # 3 TID |
|
Tamspeed Cap. |
1 Tab # 1 hs |
|
Medilac-DS Enteric Coated Cap. |
2 Tab # 2 BID |
|
Uninechol Tab. |
1 Tab # 1 hs |
|
Bolgre Cap. |
2 Tab # 2 BID |
|
Trestan Cap. |
2 Tab # 2 BID |
|
Unireba Tab. |
3 Tab # 3 TID |
7. 욕창의 평가
본 의료진은 욕창 상태 및 변화 정도를 평가하기 위하여 Braden scale 및 PUSH scale을 사용하였다. Braden scale은 일반적으로 사용하는 욕창 위험도 평가 도구로 Sensory/Mental, Moisture, Activity, Mobility, Nutrition, Friction/Shear 7가지 항목에서 1~4점까지 구성되어 각 항목 점수의 합으로 계산하며, 15~18점 Mild risk, 13~14점 Moderate risk, 10~12점 High risk, 9점 이하 Severe risk로 평가한다 12( Supplementary Material 2). Push scale(Pressure Ulcer Scale for Healing)은 NPUAP에서 개발한 욕창 상태 평가 도구로 Length x Width, Exudate Amout, Tissue type 3가지 항목으로 구성되어 각 항목 점수의 합으로 계산하며, 점수 변화를 통해 치료 효과를 평가할 수 있다 13( Supplementary Material 3). 본원 입원 시 좌측 대전자부의 욕창 크기는 6 cm ×6 cm, Braden scale 15점, PUSH scale 16점, 괴사조직은 없는 적색기로 평가되었다( Fig. 1). 입원 치료 기간 중에는 약 1~2개월 간격으로 혈액검사를 통해 혈청 알부민 수치의 변화를 평가하였다.
Fig. 1
Pressure ulcer upon admission to WKUGH.
On April 22, 2021, the pressure ulcer was diagnosed as grade IV according to the NPUAP scale. On the day of admission to WKUGH (July 08, 2021), the lesion was assessed to measure 6×6 cm in size, with the PUSH scale of 16, the Braden scale of 15, and was classified as being in the red stage. NPUAP : National Pressure Ulcer Advisory Panel, PUSH : Pressure Ulcer Scale for Healing, WKUGH : Wonkwang University Gwangju Hospital

8. 치 료
1) 침치료 및 드레싱 : 욕창 병변을 물리적으로 보호하고, 감염을 방지하며, 분비물의 흡수 및 습윤 환경을 유지하기 위한 목적으로 2021년 07월 08일부터 2022년 02월 16일까지 습윤 드레싱을 1일 1회 시행하였고, 습윤 드레싱 과정 중에 침치료가 병행되었다. 세부적인 과정은 다음과 같다. 생리식염수(대한 관류용 멸균 생리식염수, 대한약품공업주식회사)로 좌측 대전자의 욕창 병변을 닦아내고 포비돈-요오드 10% 스왑스틱((주)퍼슨)으로 소독한 후 직경 0.18 mm, 길이 8 mm의 1회용 stainless 호침(동방침구제작소, 보령시, 한국)으로 특정 경혈이 아닌 욕창 병변의 주변부에 산자(散刺) 및 점자출혈을 시행하였다( Fig. 2). 15분의 유침 후 발침하고, 생리식염수로 욕창 병변을 다시 닦아낸 뒤 메디폼(Mundipharma, 5 mm) 및 거즈를 부착하였다.
Fig. 2
Acupuncture treatment for the pressure ulcer area.
The pressure ulcer lesion was cleansed with normal saline, disinfected using a 10% povidone- iodine swab stick, and then acupuncture was performed around the lesion using a disposable stainless needle with a diameter of 0.18 mm and a length of 8 mm.

2) 한약 치료 : 약 1.5개월의 입원 치료로 인한 기력저하 호전 및 욕창 병변의 재생을 촉진하는 목적으로 가미십전대보탕( Table 2)을 2021년 08월 24일부터 하루 3회 복용하도록 처방하였다.
Table 2
Composition of a Daily Dosage of Gami-sipjeondaebo-tang (Shi-quan-da- bu-tang in Chinese, Juzentaihoto in Japanese)
|
Scientific name |
Dosage (g) |
|
Ginseng Radix (人蔘) |
9 g # 3 |
|
Atractylodis Rhizoma Alba (白朮) |
9 g # 3 |
|
Poria Sclerotium (白茯苓) |
9 g # 3 |
|
Glycyrrhizae Radix et Rhizoma (甘草) |
9 g # 3 |
|
Rehmanniae Radix Preparata (熟地黃) |
9 g # 3 |
|
Paeoniae Alba Radix (白芍藥) |
9 g # 3 |
|
Cnidii Rhizoma (川芎) |
9 g # 3 |
|
Angelicae Gigantis Radix (當歸) |
9 g # 3 |
|
Astragali Radix (黃芪) |
9 g # 3 |
|
Cinnamomi Cortex (肉桂) |
9 g # 3 |
|
Citri Unshii Pericarpium (陳皮) |
9 g # 3 |
|
Linderae Radix (烏藥) |
9 g # 3 |
|
Schisandrae Fructus (五味子) |
9 g # 3 |
|
Rhizoma Zingiberis Siccus (生薑) |
9 g # 3 |
|
Zizyphi Fructus (大棗) |
9 g # 3 |
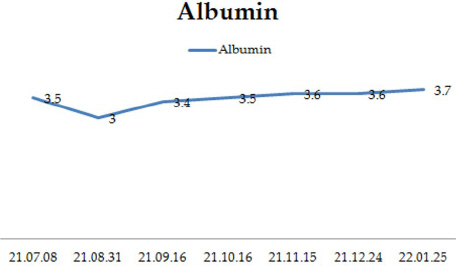
치료 경과에 따른 욕창 병변의 크기 변화 및 Braden scale, PUSH scale은 Fig. 3에 나타냈다. Braden scale은 치료 기간 중 15점에서 19점으로 상승하였으며, PUSH scale은 16점에서 0점으로 감소하였다. 환자의 보행 정도는 입원 시 휠체어를 사용하였으나, 2021년 10월경 보행기를 사용하여 보행이 가능하였고, 2021년 12월경 지팡이를 사용하여 보행이 가능한 정도로 호전되었다. 치료기간 중 시행한 혈액검사상 혈청 알부민 수치의 변화는 Fig. 4에 나타냈다. 완치 이후 2023년 08월 31일까지 추적 관찰하였으며, 욕창의 재발은 없었다.
Fig. 3
Timeline of the case.
Changes in the size of the pressure ulcer lesion according to the treatment progress, accompanied by Braden scale and PUSH scale evaluations. PUSH : pressure ulcer scale for healing
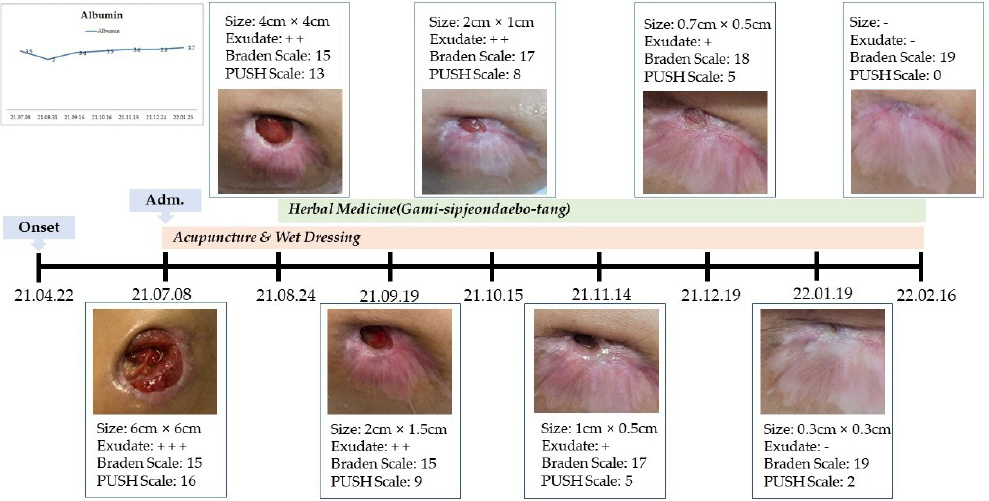
Fig. 4
III. 고찰 및 결론
본 증례는 장기간 와상으로 인해 발생한 4도 욕창 환자에게 약 7개월간 가미십전대보탕 투여 및 침치료와 습윤 드레싱의 병행을 통해 치료한 사례이다. 대상자는 성형외과에서 수술적 치료가 필요할 수도 있다는 소견을 이미 들은 상태였고, 고령이었으며, 오래된 당뇨병과 고혈압, 대변실금, 말초혈액순환 장애 등 욕창의 치유를 지연시키는 요인 6을 다수 가지고 있었음에도 불구하고 완치되었으며, 완치 이후 1년 6개월의 추적관찰기간 동안 재발도 없었다. 한의학의 외과서 중 하나인 ≪瘍醫大全≫에서는 욕창의 원인, 발병부위, 치료에 대해 상세히 기술하고 있다 1. 치료방법 중 내치법(內治法)의 치료원칙으로 보익기혈(補益氣血), 화영탁독(和營托毒)을, 상용약물로는 황기, 백출, 당삼, 복령, 당귀, 적작약, 단삼 등을 제시하였다 1. 실제로 욕창에 대한 한의치료 증례에서 가장 많이 사용된 처방은 氣血虛의 대표방인 십전대보탕이었으며 1, 본 증례 역시 가미십전대보탕을 사용하였다. 한약치료와 침치료가 욕창을 포함한 상처 회복에 유의미한 효과가 있음을 제시한 연구는 상당수 존재한다. 신 등 14은 쥐를 이용한 모세혈관투과성실험, 육아종 형성실험 및 섬유아세포의 증식능에 대한 실험을 통해 십전대보탕이 생기(生肌)작용에 효과가 있음을 보고하였으며, 정 등 15은 실험연구를 통해 십전대보탕이 혈액 내 면역세포를 줄여 상처의 치유를 돕고, TNF-α, IL-1β 같은 혈액 내의 염증 사이토카인과 염증매개 인자 발현을 억제하는 항염증 효과와 콜라겐의 증착과 만성염증으로의 진행을 억제하는 효과가 있음을 제시하였다 15. 이 등 16은 상처 부위의 침치료가 유의미하게 basic fibroblast growth factor(bFGF)를 증가시킴으로써 상처 재생을 촉진하는 효과가 있다고 보고하였다. bFGF는 흉터의 형성을 유도하는 α-SMA를 감소시키고, 상처 치유에 중요한 역할을 하는 fibronectin은 증가시키는 역할을 한다 16. 본 증례의 결과 역시 이러한 기존 연구들에서 밝힌 기전으로 설명할 수 있을 것으로 사료된다. 본 연구의 한계점은 다음과 같다. 첫째, 욕창의 완치가 자연회복, 혹은 습윤 드레싱의 단독 효과에 의한 것은 아닌지를 완전히 배제할 수 없다. 하지만 본 증례에 사용된 십전대보탕과 침치료가 상처 회복에 관여하는 기전이 여러 연구 14-16에서 보고된 바 있으므로 자연회복, 혹은 습윤 드레싱의 단독 효과일 가능성은 낮을 것으로 사료된다. 둘째, 욕창 발병 당일부터 한의과 치료를 받은 증례는 아니며, Braden scale 상으로는 15점으로 mild risk에 속했다는 점이다. 본 증례의 대상자는 4도 욕창 진단 후 약 2.5개월간 타병원에서 치료를 받고, 이후에 적극적인 치료를 위해 본원에 내원하였다. 하지만 일반적으로 4도 욕창은 치료를 받더라도 완화는 가능하나, 완치는 어렵다는 점 5에서 완치를 이끌어낸 본 증례의 의의는 작지 않을 것으로 사료된다. 셋째, 1례에 불과하며, 유사한 보고들이 존재한다. 하지만 본 증례의 대상자는 고령이면서 20년 이상된 당뇨병과 고혈압, 대변실금, 하지 부종과 저림 등 말초순환장애 의심 소견과 같은 욕창의 치유를 지연시키는 다양한 요인을 가지고 있었음에도 불구하고 완치가 됐다. 또한 본 연구처럼 욕창 완치 후에도 1년이 넘는 기간 동안 욕창의 재발을 평가한 연구는 없다. 본 증례는 이러한 한계점에도 불구하고 대전자 부위의 4도 욕창을 한의 치료와 습윤 드레싱 요법의 병행을 통해 수술적 치료 없이 완치시켰고, 이후 1년 6개월 동안 재발이 없는 것을 추적관찰하였기에 보고하는 바이다.
감사의 글
This paper was supported by Wonkwang University in 2023.
참고문헌
1. Kim JY, Kim HG, Kim SG, Lim SH. A Review on Decubitus Ulcer Treatment in Korean Medicine. J Korean Med Ophthalmol Otolaryngol Dermatol 2019:32(3):87–104.
2. Park JM, Kim YS, Kim HS, Kim JT, Kim SK. Clinical Consideration of the Pressure Sore. Archives of Plastic Surgery 1997:24(5):1194–206.
4. Oh KS, Lim SY, Mun GH, Hyon WS, Bang SI. The Treatment of Pressure Sore. J Korean Wound Care Soc 2005:1(1):83–6.
5. Seo JB, Lee TJ, Lee JW, Kim KA, Yoon JJ. 9 Cases of Pressure Ulcers Cured by Acupuncture Treatment and Open Wet Dressing Therapy. J Physiol &Pathol Korean Med 2020:34(5):269–78.  6. Park KH. Factors Affecting the Healing of Pressure Ulcers. J Korean Wound Management Soc 2008:4(2):92–5.
7. Kim K, Lee YU, Kim CH, Lim HS, Kang G, Lee S. Case Report of Korean Medicine Treatment and Dressing Therapy for Grade III Trochanteric Pressure Sore. J Int Korean Med 2021:42(2):122–30.  8. Jeong HS, Kim HR, Kim SY, Lee SW, Cho SY, Ko CN, et al. A Clinical Case Report on Grade Four Pressure Ulcer Patients Treated with Hwangryunhaedok-tang Pharmacopuncture and Herbal Medicine Taklisodok-eum. The Journal of the Society of Stroke on Korean Medicine 2019:20(1):65–74.
9. Ryu HR, Kang EJ, Kim YK, Kim KM. A Case Report of Stage 4 Pressure Ulcer Patient Treated with Acupuncture and the Herbal Medicine Gamisipjeon-tang. J Int Korean Med 2017:38(5):619–27. 10. Lee DH, Nam JS, Jeong HS, Jang IS, Seo ES. Two Cases of Grade Four Pressure Ulcer Patients Treated with Pharmacopuncture Soyeom and Herbal Medicine Taklisodok-eum. J Int Korean Med 2010:31(2):200–6.
11. Park CS, Heo CY. Prevention and Treatment of Pressure Ulcers. Korean Med Assoc 2015:58(9):786–94. 12. Braden BJ. The Braden scale for predicting pressure sore risk:reflections after 25 years. Advances in skin &wound care 2012:25(2):61.
13. Choi EP, Chin WY, Wan EY, Lam CL. Evaluation of the Internal and External Responsiveness of the Pressure Ulcer Scale for Healing (PUSH) Tool for Assessing Acute and Chronic Wounds. Journal of Advanced Nursing 2016:72(5):1134–43.  14. Shin MH, Ro SS, Kim BT. Effect of Sip-Jeon- Dae-Bo-Tang (SJDBT) Extract on Wound Healing. J of Korean medicine 1993:14(1):31–44.
15. Jung H, Lee HJ, Kim B, Lee CH, Lee EJ, Heo DS, et al. The Effects of Sibjeondaebotanggamibang on the Treating of Wound. Journal of Korean Medicine Rehabilitation 2014:24(3):51–69.
16. Lee JA, Jeong HJ, Park HJ, Jeon S, Hong SU. Acupuncture Accelerates Wound Healing in Burn-injured Mice. Burns 2011:37(1):117–25.
Appendices
【Supplementary Meterial 1】
National Pressure Ulcer Advisory Panel(NPUAP) Pressure Injury Stages
|
Grade |
Definition |
|
Stage 1 |
Intact skin with non-blanchable redness of a localized area usually over a bony prominence Darkly pigmented skin may not have visible blanching; its color may differ from the surrounding area |
|
|
Stage 2 |
Partial thickness loss of dermis presenting as a shallow open ulcer with a red pink wound bed, without slough May also present as an intact or open/ruptured serum-filled blister |
|
|
Stage 3 |
Full thickness tissue loss Subcutaneous fat may be visible but bone, tendon or muscle are not exposed Slough may be present but does not obscure the depth of tissue loss May include undermining and tunneling |
|
|
Stage 4 |
Full thickness tissue loss with exposed bone, tendon or muscle Slough or eschar may be present on some parts of the wound bed Often include undermining and tunneling |
|
|
Suspected Deep Tissue Injury |
Purple or maroon localized area of discolored intact skin or blood-filled due to damage of underlying soft tissue from pressure and/or shear The area may be preceded by tissue that is painful, firm, mushy, boggy, warmer or cooler as compared to adjacent tissue |
|
|
Unstageable |
Full thickness tissue loss in which the base of the ulcer is covered by slough (yellow, tan, gray, green or brown) and/or eschar (tan, brown, or black) in the wound bed |
【Supplementary Material 2】
|
Scale |
Sensory/ Mental |
Moisture |
Activity |
Mobility |
Nutrition |
Friction/ Shear |
|
1 |
Totally limited |
Constantly moist |
Bedfast |
100% immobile |
Very poor |
Frequent sliding |
|
|
2 |
Very limited |
Very moist |
Chairfast |
Very limited |
<1/2 daily portion |
Feeble corrections |
|
|
3 |
Slightly limited |
Occasionally moist |
Walks with assistance |
Slightly limited |
Most of portion |
Independant corrections |
|
|
4 |
No impairment |
Dry |
Walks without assistance |
Full mobility |
Eats everything |
|
【Supplementary Material 3】
The Pressure Ulcer Scale for Healing (PUSH Tool)
|
Length× Width (in cm2) |
0 0 |
1 <0.3 |
2 0.3-0.6 |
3 0.7-1.0 |
4 1.1-2.0 |
5 2.1-3.0 |
Sub-score |
|
|
6 3.1-4.0 |
7 4.1-8.0 |
8 8.1-12.0 |
9 12.1-24.0 |
10 >24.0 |
|
|
Exudate Amount |
0 None |
1 Light |
2 Moderate |
3 Heavy |
|
|
Sub-score |
|
|
Tissue type |
0 Closed |
1 Epithelial Tissue |
2 Granulation Tissue |
3 Slough |
4 Necrotic Tissue |
|
Sub-score |
|
|
|
|
|
|
|
|
Total score |
|
|