Kim, Park, Park, Kim, and Ko: Herbal Medicine for the Treatment of Non-Erosive Reflux Disease: A Systematic Review and Meta-Analysis Protocol
Abstract
Introduction:
Non-erosive reflux disease (NERD) is the most common subtype of gastroesophageal reflux disease (GERD). This study aims to synthesize evidence on the efficacy and safety of various herbal medicines for the treatment of NERD.
Methods and analysis:
Ten electronic databases will be examined: MEDLINE (via PubMed), Cochrane Central Register of Controlled Trials, Embase, Allied and Complementary Medicine Database, China National Knowledge Infrastructure Database, Citation Information by Nii, Korean Medical Database, Korean Studies Information Service System, National Digital Science Library, and Oriental Medicine Advanced Searching Integrated System. All randomized controlled trials published from inception to May 2023 that meet the eligibility criteria will be selected. Two independent researchers will extract data, such as publication year, study design, intervention details, outcome measures, main results, and adverse events. The risk of bias and quality of evidence will be assessed, and subgroup analyses will be performed according to the type of control intervention and herbal medicine. The analysis process will be conducted using Review Manager 5.4 software.
Discussion:
This review will present a summary and rationale for herbal medicine’s effectiveness in treating NERD. The findings of this review can help those who want to apply herbal medicine to the treatment of NERD.
Systematic review registration:
PROSPERO registration number CRD42023423052.
KeywordsKeywords: Non-erosive reflux disease, Herbal Medicine, Systematic Review, Meta-Analysis
I. Introduction
Gastroesophageal reflux disease (GERD) is one of the most commonly diagnosed chronic gastrointestinal disorders and is characterized by regurgitation of stomach contents back into the esophagus. Based on the endoscopic and histopathological appearance, there are several phenotypes of GERD, such as non-erosive reflux disease (NERD), erosive esophagitis, and Barrett’s esophagus. NERD accounts for the most prevalent type among them 1. Symptoms induced by the regurgitation of gastric juice associated with NERD, even without inflammatory lesions on the mucous membrane of the esophagus, can contribute to lowering the patients’ quality of life and generating severe heartburn 2,3. Conventional treatment options currently include lifestyle modifications, medical, surgical, and endoluminal therapy 4. Proton pump inhibitor (PPI) therapy is the most widely used method that can be tried in medical therapy. However, evidence for the effectiveness of PPIs in the treatment of NERD has not been sufficiently established 5,6. Herbal medicine can serve as a viable alternative for treating NERD, particularly when Western medicine fails to provide desired results, such as in cases of PPI-refractory reflux disease or when dose reduction is preferred. There have been various types of reports, such as case reports, randomized controlled trials (RCT), and systematic reviews that confirmed the efficacy and safety of herbal medicine treatment on GERD and NERD 7-10. A meta-analysis confirming the efficacy and safety of traditional treatment of NERD was conducted in 2018 11. However, the databases searched were limited to English and Chinese, and trials involving Western medicine in the intervention group were excluded. Therefore, we aimed to search for more recent and extensive trials relevant to herbal medicine treatment of NERD and conduct subgroup analyses to synthesize the current state of evidence on the efficacy of herbal medicine in treating NERD.
II. Methods and analysis
This systematic review and meta-analysis aimed to identify, synthesize, and analyze the evidence on the efficacy and safety of herbal medicines for NERD. The systematic review and meta-analysis will be conducted according to the Cochrane Handbook for Systematic Reviews of Interventions 12. The protocol for this systematic review is based on the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) guideline 13, and is registered in the International Prospective Register of Systematic Review (PROSPERO) with registration number CRD42023423052.
1. Search strategy
We will search the following 10 electronic databases from inception to May 2023 without language or publication date restrictions: MEDLINE (via PubMed), Cochrane Central Register of Controlled Trials (CENTRAL), Embase, Allied and Complementary Medicine Database (AMED), China National Knowledge Infrastructure Database (CNKI), Citation Information by Nii (CiNii), Korean Medical Database (Kmbase), Korean Studies Information Service System (KISS), National Digital Science Library (NDSL), Oriental Medicine Advanced Searching Integrated System (OASIS). The search term will consist of a combination of controlled terms such as Medical Subject Headings (MeSH) and free text words related to “non-erosive reflux disease”, “herbal medicine”, or “traditional medicine”. The search strategy for MEDLINE is shown in Table 1.
Table 1
Search strategy for Medline via PubMed
|
No. |
Search strategy |
|
#1. |
gastroesophageal reflux[MeSH Terms] |
|
|
#2. |
gastric acid reflux[tiab] OR acid reflux, gastric[tiab] OR reflux, gastric acid[tiab] OR gastric acid reflux disease[tiab] |
|
|
#3. |
gastro-esophageal reflux disease[tiab] OR gastro esophageal reflux disease[tiab] OR gastro-esophageal reflux diseases[tiab] OR reflux disease, gastro-esophageal[tiab] |
|
|
#4. |
gastro-oesophageal reflux[tiab] OR gastro oesophageal reflux[tiab] OR reflux, gastro-oesophageal[tiab] |
|
|
#5. |
gastroesophageal reflux disease[tiab] |
|
|
#6. |
GERD[tiab] OR reflux, gastroesophageal[tiab] OR esophageal reflux[tiab] OR gastro-esophageal reflux[tiab] OR gastro esophageal reflux[tiab] OR reflux, gastro-esophageal[tiab] |
|
|
#7. |
#1 OR #2 OR #3 OR #4 OR #5 OR #6 |
|
|
#8. |
non erosive[tiab] OR non-erosive[tiab] OR nonerosive[tiab] OR non erosion[tiab] OR non-erosion[tiab] OR NERD[tiab] OR non erosive reflux disease[tiab] OR non-erosive reflux disease[tiab] OR nonerosive reflux disease[tiab] OR non erosion reflux disease[tiab] OR non-erosion reflux disease[tiab] |
|
|
#9. |
#7 OR #8 |
|
|
#10. |
herbal medicine[MeSH Terms] |
|
|
#11. |
medicine, herbal[tiab] OR herb*[tiab] |
|
|
#12. |
plants, medicinal[MeSH Terms] OR plant extracts[MeSH Terms] |
|
|
#13. |
medicine, traditional[MeSH Terms] OR medicine, korean traditional[MeSH Terms] OR medicine, chinese traditional[MeSH Terms] OR medicine, east asian traditional[MeSH Terms] |
|
|
#14. |
korean[tiab] OR chinese[tiab] OR east asian[tiab] OR japanese[tiab] |
|
|
#15. |
tradition*[tiab] |
|
|
#16. |
#14 AND #15 |
|
|
#17. |
traditional[tiab] OR chinese[tiab] OR herbal[tiab] |
|
|
#18. |
medicine[tiab] |
|
|
#19. |
#17 AND #18 |
|
|
#20. |
medicine, kampo[MeSH Terms] |
|
|
#21. |
complementary therapies[MeSH Terms] |
|
|
#22. |
drugs, chinese herbal[MeSH Terms] |
|
|
#23. |
tang[tiab] OR decoction[tiab] OR formula*[tiab] OR herbal formula[tiab] OR granule[tiab] OR syrup[tiab] OR san[tiab] OR hwan[tiab] OR capsule[tiab] OR powder[tiab] OR tablet[tiab] |
|
|
#24. |
#10 OR #11 OR #12 OR #13 OR #16 OR #19 OR #20 OR #21 OR #22 OR #23 |
|
|
#25. |
randomized controlled trial[pt] |
|
|
#26. |
controlled clinical trial[pt] |
|
|
#27. |
randomized[tiab] OR randomised[tiab] |
|
|
#28. |
randomly[tiab] |
|
|
#29. |
clinical[tiab] |
|
|
#30. |
trial*[tiab] |
|
|
#31. |
clinical trial[tiab] |
|
|
#32. |
#25 OR #26 OR #27 OR #28 OR #29 OR #30 OR #31 |
|
|
#33. |
#9 AND #24 AND #32 |
2. Eligibility criteria
The following eligibility criteria will be applied to select the appropriate studies for inclusion in this review.
1) Types of studies
RCTs and quasi-RCTs in humans will be included. Other than RCTs, such as case reports, retrospective studies, reviews, and animal studies will be excluded.
2) Types of participants
Patients diagnosed with NERD will be included, and those diagnosed with any organic disease associated with symptoms other than GERD or NERD will be excluded. There will be no restriction on demographic characteristics, such as race or gender, but studies involving only non-adults under the age of 19 years will be excluded.
3) Types of interventions
Studies involving any type of herbal medicine, such as a decoction, pill, tablet, capsule, or powder administered orally as an intervention, will be included. There will be no restrictions on the number of herbs that comprise the formula, and studies using herbal medicines consisting of only one herb as an intervention will also be included. Studies comparing herbal medicine with any type of control intervention will be included: herbal medicine alone, herbal medicine combined with Western medicine versus Western medicine alone, herbal medicine versus placebo formulation, and herbal medicine versus no treatment. However, studies that involved other traditional treatment methods, such as acupuncture or moxibustion with herbal medicine as the main intervention in the treatment group and studies that included herbal medicine as an intervention in both the control and treatment groups, will be excluded.
4) Types of outcome measures
The primary outcome will be the total efficacy rate. Symptom scores and quality of life examined by self-response questionnaires such as reflux diagnostic questionnaire score, gastroesophageal reflux disease questionnaire, short-form 36 health survey score, and recurrence rates will be secondary outcomes.
3. Study selection
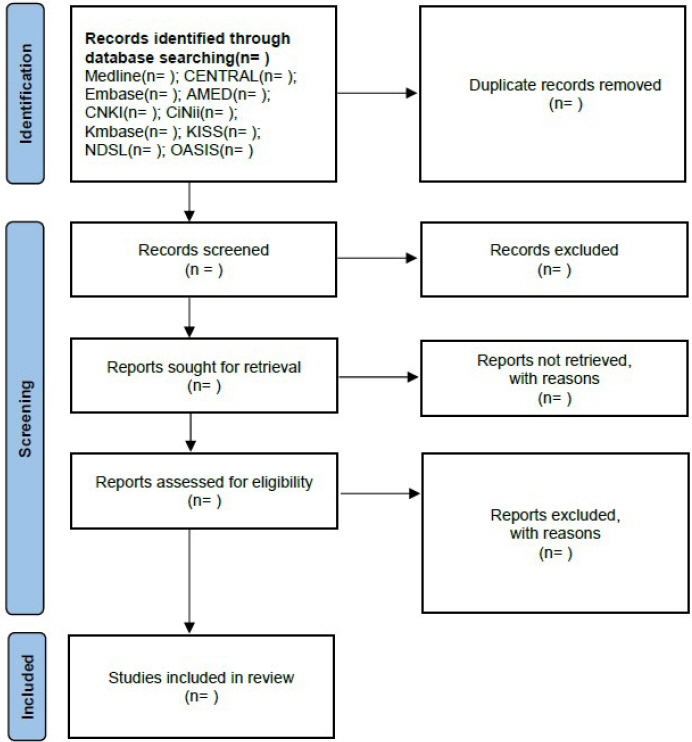
Two researchers (MK and CP) will independently examine the titles and abstracts of all retrieved studies in the first phase of screening. In the second phase, researchers will undergo a full-text screening process. Disagreements between the two researchers will be resolved through a discussion with a senior researcher (S-JK). Duplicates among the studies will be identified by study characteristics such as author names, publication year, trial registration number, intervention, or participants during the screening process, and multiple reports will be removed. The selection process will be shown in the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) flow diagram ( Fig. 1). Selected studies that meet the eligibility criteria above will undergo data extraction process. Data management will be performed using Endnote X20 software program.
Fig. 1
Flow chart of the search process.
CENTRAL : Cochrane Central Register of Controlled Trials, AMED : Allied and Complementary Medicine Database, CNKI : China National Knowledge Infrastructure Database, CiNii : Citation Information by Nii, Kmbase : Korean Medical Database, KISS : Korean Studies Information Service System, NDSL : National Digital Science Library, OASIS : Oriental Medicine Advanced Searching Integrated System
4. Data extraction
Data extraction will be performed by two independent researchers (MK and CP), and data will be recorded in a pre-defined form. The extracted data will include the basic characteristics of the study, such as authors’ name, year of publication, study design, information about participants, details of the intervention, outcome measures, main results, and adverse events. Details of the intervention will include the type of herbal medicine, and duration and frequency of treatment.
III. Meta-analysis
1. Assessment of the risk of bias
The quality of all selected studies will be assessed using the Cochrane risk-of-bias tool for randomized trials individually 14. Biases in the random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, and selective reporting will be checked. Each domain will be judged as low, uncertain, or high.
2. Data synthesis and analysis
Results such as the overall efficacy rate from the treatment and control groups will be compared. Dichotomous data will be presented as risk ratios (RR) with a 95% confidence intervals (CI); continuous data will be presented as mean difference (MD) or standardized mean difference (SMD) with a 95% CI 15. Statistical analyses will be conducted using Review Manager program (RevMan) version 5.4.. A narrative summary will be provided if the studies are not appropriate for quantitative synthesis. Statistical heterogeneity of the studies will be measured using I2 statistics; if it is over 50%, it will be considered to have significant heterogeneity 16. Fixed- or random- effects models will be used for the meta-analysis. In addition, a funnel plot will be used to assess publication bias in terms of the primary outcome.
3. Assessment of meta-biases
The quality of evidences from the included studies will be assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) framework. The risks of bias, imprecision, inconsistency, indirectness, and publication bias will be assessed and graded as high, moderate, low, or very low 17.
4. Subgroup analyses
A subgroup analysis will be performed based on the type of control intervention or type of herbal medicine used. Differences will be compared according to the type of Western medicine and whether herbal medicine is combined with Western medicine or used alone.
IV. Discussion
NERD is the most common type of GERD. It is defined as the absence of mucosal lesions confirmed by endoscopy and represents up to 60% of all patients with reflux symptoms 18. Medical treatment of patients with NERD is based on gastric acid- suppressive drugs such as PPIs. Although PPI therapy is the most effective method for treating GERD, the response rates to PPIs are lower in patients than in those with other phenotypes of GERD 19. This systematic review and meta-analysis will assess the efficacy and safety of herbal medicines for the treatment of NERD. Herbal medicines can be a helpful option for the treatment of reflux disease, especially in cases that do not respond to conventional medical treatments, including proton pump inhibitors. Various herbal medicines can alleviate the symptoms of non-erosive reflux disease in patients with symptoms such as heartburn 20,21. In this study, we will investigate clinical trials published from the inception of herbal medicine treatment for NERD, and synthesize recent evidence of its efficacy.
Ethics and dissemination
Since this study do not include individual patient data, ethical approval is not required. The results of this systematic review will be disseminated via peer-reviewed journal publication or conference presentations.
Acknowledgements
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Contributors
Both MK and CP contributed to the conceptualization of the review. Both J-WP and JK contributed to the development of the search strategy and design of the analysis plan. MK wrote the initial draft of the manuscript. S-JK reviewed and edited the final manuscript. All the authors have read and approved the final version of the manuscript.
Funding
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2022R1C1C1004937) to S.J.K..
This funding source had no role in the design of this study and will not play any role during its execution, analysis, interpretation of the data, or decision to submit the results.
References
2. Zhang JX, Ji MY, Song J, Lei HB, Qiu S, Wang J, et al. Proton Pump Inhibitor for Non-Erosive Reflux Disease:A Meta-Analysis. World J Gastroenterol 2013:19(45):8408–19.    3. El-Serag HB, Sweet S, Winchester CC, Dent J. Update on the Epidemiology of Gastro-Oesophageal Reflux Disease:A Systematic Review. Gut 2014:63(6):871–80. 4. Antunes C, Aleem A, Curtis SA. Gastroesophageal Reflux Disease. StatPearls [Internet] 2023:
5. Scarpignato C. Poor Effectiveness of Proton Pump Inhibitors in Non-Erosive Reflux Disease:The Truth in the End! Neurogastroenterol Motil 2012:24(8):697–704. 6. Woodland P, Sifrim D. Management of Gastro- Oesophageal Reflux Disease Symptoms That Do Not Respond to Proton Pump Inhibitors. Curr Opin Gastroenterol 2013:29(4):431–6. 7. Sadeghi F, Mohammad S, Sepehri B, Khodaie L, Monirifar H, Mirghafourvand M. Effects of Herbal Medicine in Gastroesophageal Reflux Disease Symptoms:A Systematic Review and Meta-Analysis. Tradit Med Res 2020:5(6):464–75. 8. Tominaga K, Iwakiri R, Fujimoto K, Fujiwara Y, Tanaka M, Shimoyama Y, et al. Rikkunshito Improves Symptoms in PPI-Refractory GERD Patients:A Prospective, Randomized, Multicenter Trial in Japan. J Gastroenterol 2012:47(3):284–92.  10. Los UMDECDE. A Clinical Case Report of Non- Erosive Reflux Disease Treated with Traditional Oriental Medicine. Korean J Orient Intern Med 2006:27(4):991–8.
12. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, et al. Cochrane Handbook for Systematic Reviews of Interventions Version 6.3(Updated August 2022). Cochrane 2022:
13. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 Statement:An Updated Guideline for Reporting Systematic Reviews. BMJ 2021:372.
14. Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2:A Revised Tool for Assessing Risk of Bias in Randomised Trials. BMJ 2019:366:1–8. 15. Andrade C. Understanding Relative Risk, Odds Ratio, and Related Terms:As Simple as It Can Get. J Clin Psychiatry 2015:76(7):e857–61. 16. Melsen WG, Bootsma MC, Rovers MM, Bonten MJ. The Effects of Clinical and Statistical Heterogeneity on the Predictive Values of Results from Meta-Analyses. Clin Microbiol Infect 2014:20(2):123–9. 17. Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE:An Emerging Consensus on Rating Quality of Evidence and Strength of Recommendations. BMJ 2008:336(7650):924–6. 18. Karamanolis GP, Tutuian R. Role of Non-Acid Reflux in Patients with Non-Erosive Reflux Disease. Ann Gastroenterol 2013:26(2):100–3. 19. Sigterman KE, van Pinxteren B, Bonis PA, Lau J, Numans ME. Short-Term Treatment with Proton Pump Inhibitors, H2-Receptor Antagonists and Prokinetics for Gastro-Oesophageal Reflux Disease-like Symptoms and Endoscopy Negative Reflux Disease. Cochrane Database Syst Rev 2013:2013(5):CD002095. 20. Tominaga K, Kato M, Takeda H, Shimoyama Y, Umegaki E, Iwakiri R, et al. A Randomized, Placebo-Controlled, Double-Blind Clinical Trial of Rikkunshito for Patients with Non-Erosive Reflux Disease Refractory to Proton-Pump Inhibitor:The G-PRIDE Study. J Gastroenterol 2014:49(10):1392–405. 21. Li BS, Li ZH, Tang XD, Zhang LY, Zhao YP, Bian LQ, et al. A Randomized, Controlled, Double-Blinded and Double-Dummy Trial of the Effect of Tongjiang Granule on the Nonerosive Reflux Disease of and Gan-Wei Incoordination Syndrome. Chin J Integr Med 2011:17(5):339–45.
Appendices
【PRISMA-P (Preferred Reporting Items for Systematic review and Meta-Analysis Protocols) 2015 checklist : recommended items to address in a systematic review protocol *】
|
Section and topic |
Item No |
Checklist item |
Reported on Page # |
|
ADMINISTRATIVE INFORMATION |
|
Title : |
|
Identification |
1a |
Identify the report as a protocol of a systematic review |
1 |
|
Update |
1b |
If the protocol is for an update of a previous systematic review, identify as such |
N/A |
|
Registration |
2 |
If registered, provide the name of the registry (such as PROSPERO) and registration number |
2 |
|
Authors : |
|
Contact |
3a |
Provide name, institutional affiliation, e-mail address of all protocol authors; provide physical mailing address of corresponding author |
1 |
|
Contributions |
3b |
Describe contributions of protocol authors and identify the guarantor of the review |
11 |
|
Amendments |
4 |
If the protocol represents an amendment of a previously completed or published protocol, identify as such and list changes; otherwise, state plan for documenting important protocol amendments |
N/A |
|
Support : |
|
Sources |
5a |
Indicate sources of financial or other support for the review |
12 |
|
Sponsor |
5b |
Provide name for the review funder and/or sponsor |
12 |
|
Role of sponsor or funder |
5c |
Describe roles of funder(s), sponsor(s), and/or institution(s), if any, in developing the protocol |
12 |
|
INTRODUCTION |
|
Rationale |
6 |
Describe the rationale for the review in the context of what is already known |
3 |
|
Objectives |
7 |
Provide an explicit statement of the question(s) the review will address with reference to participants, interventions, comparators, and outcomes (PICO) |
3 |
|
METHODS |
|
Eligibility criteria |
8 |
Specify the study characteristics (such as PICO, study design, setting, time frame) and report characteristics (such as years considered, language, publication status) to be used as criteria for eligibility for the review |
3-7 |
|
Information sources |
9 |
Describe all intended information sources (such as electronic databases, contact with study authors, trial registers or other grey literature sources) with planned dates of coverage |
3-4 |
|
Search strategy |
10 |
Present draft of search strategy to be used for at least one electronic database, including planned limits, such that it could be repeated |
5-6 |
|
Study records: |
|
Data management |
11a |
Describe the mechanism(s) that will be used to manage records and data throughout the review |
7-8 |
|
Selection process |
11b |
State the process that will be used for selecting studies (such as two independent reviewers) through each phase of the review (that is, screening, eligibility and inclusion in meta-analysis) |
7-8 |
|
Data collection process |
11c |
Describe planned method of extracting data from reports (such as piloting forms, done independently, in duplicate), any processes for obtaining and confirming data from investigators |
10 |
|
Data items |
12 |
List and define all variables for which data will be sought (such as PICO items, funding sources), any pre-planned data assumptions and simplifications |
10 |
|
Outcomes and prioritization |
13 |
List and define all outcomes for which data will be sought, including prioritization of main and additional outcomes, with rationale |
10 |
|
Risk of bias in individual studies |
14 |
Describe anticipated methods for assessing risk of bias of individual studies, including whether this will be done at the outcome or study level, or both; state how this information will be used in data synthesis |
10 |
|
Data synthesis |
15a |
Describe criteria under which study data will be quantitatively synthesised |
10 |
|
15b |
If data are appropriate for quantitative synthesis, describe planned summary measures, methods of handling data and methods of combining data from studies, including any planned exploration of consistency (such as I2, Kendall’s τ) |
10 |
|
15c |
Describe any proposed additional analyses (such as sensitivity or subgroup analyses, meta-regression) |
10-11 |
|
15d |
If quantitative synthesis is not appropriate, describe the type of summary planned |
10 |
|
Meta-bias(es) |
16 |
Specify any planned assessment of meta-bias (es) (such as publication bias across studies, selective reporting within studies) |
10 |
|
Confidence in cumulative evidence |
17 |
Describe how the strength of the body of evidence will be assessed (such as GRADE) |
10 |
From: Shamseer L, Moher D, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart L, PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015 Jan 2;349(jan02 1):g7647.
Pre-defined Data Extraction Form
|
No. |
First author (year) |
Language |
Participants (n) |
M:F |
Diagnosis criteria |
Invervention (n) |
Control (n) |
Treatment period |
Outcome measure |
Main results |
Side effects |
|
Age |
Content |
Content |
Main statistics |
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|