





I. 서 론
뇌졸중은 세계보건기구(World Health Organization, WHO)에서 ‘갑작스럽게 진행하는 국소적인 또는 완전한 뇌기능장애가 24시간 이상 지속하거나 심한 경우에는 사망에 이르는 질환으로, 뇌혈관의 병 이외 다른 원인이 없는 경우’로 정의한다1. 뇌졸중의 회복은 손상 받은 부위나 범위, 신경계 증상 정도, 나이, 동반 질환 등 환자 상태에 따라 편차를 보이지만1, 각 시기(stage)별 자발적 회복의 특성을 보인다. Berhardt J 등2이 정리한 기준에 따르면 발병 후 7일 이내를 급성기, 발병 후 일주일부터 6개월까지를 아급성기, 6개월 이후를 만성기로 분류한다. 뇌졸중 후 나타나는 증상 중 특히 운동 관련 증상은 발병 후 첫 몇 주 동안 현저하게 개선되고, 3개월 사이 많은 회복이 이루어지며, 이후 비교적 회복 속도가 더뎌지기는 하나 6개월까지 추가적인 개선이 이루어지고, 6개월 후에는 자연회복 속도가 상당히 감소면서 초기 대부분의 회복이 발병 후 6개월 사이에 이루어진다고 한다3,4. 이렇게 시기별로 치료 효과 속도에 차이가 있는 것은 발병 24시간 이내에 세포의 사멸, 그리고 출혈성 뇌졸중에 한하여서는 혈종의 확장이 일어난 후, 발병 일주일 내외로 염증반응과 염증수복반응을 거치고, 발병 일주일 내외로부터 내인성 가소성 원리에 따라 신경 회복이 활발히 일어나기 시작하며, 점차로 3개월부터 6개월, 그리고 6개월 이후에는 손상된 움직임이나 기능적 활동들의 회복이 이루어지는 생물학적 회복 흐름에 기초한다2,5. 이러한 뇌졸중 후 회복 과정의 시간 의존성에 대한 관점은 치료 효과를 최대화하기 위해 중요하다2.
뇌졸중 후 신경학적 회복이 일어나면서 신경학적 징후는 줄어들고 환자는 더 복합적이고 전신적인 증상들을 경험하기 때문에 환자가 처해있는 뇌졸중 시기에 맞는 적절한 평가척도가 요구된다6. 일부 평가척도는 특정 뇌졸중 시기에 목적성을 가지고 사용되기 때문에 해당 시기에만 권고되기도 한다. 예를 들어 National Institutes of Health Stroke Scale(NIHSS)은 허혈성 뇌졸중에서 신경학적 결손을 측정하기 위한 정량적 도구로, 발병 당시의 중증도를 평가하여 사망률, 기능장애, 입원 기간 및 회복의 예후를 추정하는 도구이다6,7. 그래서 NIHSS는 주로 급성기 평가척도로 사용되고, 만성기 평가척도로는 타당도가 부족하다8 Mini-Mental State Examination(MMSE)9은 본래 치매나 섬망을 선별하기 위해 만들어진 평가척도로 뇌졸중의 인지영역의 손상에서도 사용되고 있으나, 2주 이내의 초기 뇌졸중 환자에서는 흔히 추론과 집행기능에 더하여 시각적 인식과 구성 등 보다 복합적인 인지기능의 손상을 나타나기 때문에 특히 급성기 뇌졸중 인지기능장애에서의 선별 도구로 사용할 때에는 주의해서 해석해야 한다고 한다10.
그러나 국내 한의 뇌졸중 후유증 치료 임상 연구들에서 뇌졸중 시기에 대해서 명확히 언급하지 않은 경우가 있었고, 시기별로 평가척도를 적절하게 사용하지 못하고 있는 경우도 있었다. 뇌졸중 시기를 구분하고 언급하는 것이 중요한 이유는 뇌졸중 후 증상의 회복이 시간 의존적이며3, 시기별로 적용하는 한・양방의 치료 전략이 달라지기 때문이고11-16, 문헌의 체계적 분석을 통한 지식의 통합 과정에서도 서로 다른 여러 연구의 결과를 쉽게 분류하고 비교할 수 있기 때문이다. 이처럼 시기를 명확하게 보고하지 않거나 누락할 경우 후속 연구에 제한을 주게 되고, 시기의 모호한 기술이 임상에서의 활용도도 낮추게 된다.
이에 저자는 국내 한의 뇌졸중 연구를 분석하여 뇌졸중 시기에 대한 보고의 충실도 및 해당 시기에 활용된 평가척도의 적절성을 검토하고자 하였고, 한의약 뇌졸중 임상 연구에서 제시된 핵심 평가 지표를 기준으로 그 활용도를 파악해보고자 하였다. 이를 통해 향후 국내 한의 뇌졸중 후유증 치료 임상 연구에서 뇌졸중 시기에 대한 적극적 보고와 시기 적절한 임상 평가척도의 적극적 활용에 대한 제언을 담고자 하였다.
II. 연구방법
1. 연구 범주
본 연구는 WHO에서 정의한 뇌졸중을 대상으로 하였다. 뇌출혈과 뇌경색을 모두 포함하였으나, 신경계 증상이 24시간 이내에 완전히 회복되는 일과성허혈발작과 외상성으로 발병한 뇌 손상은 뇌졸중과 별도로 분류되기에1 제외하였다.
뇌졸중 후유증으로는 운동기능장애가 대부분이며, 인지기능장애, 시각지각장애, 언어장애, 강직, 삼킴곤란, 배뇨・배변장애, 수면장애, 기분장애 등이 있고, 중추성 뇌졸중 후 통증(Central post-stroke pain, CPSP)이나 어깨의 아탈구로 인한 통증, 낙상과 골절, 흡인성 폐렴, 욕창 등의 합병증도 흔히 동반된다1. 이러한 다양한 내과적, 신경학적 증상들 중 본 연구는 부전마비, 완전마비, 보행장애, 마비 후 강직, 운동실조, 진전 등 운동 관련 후유증이 있는 연구만을 대상으로 하였다.
2. 문헌 검색
국내 논문 데이터베이스 중 한국과학기술정보연구원(https://scienceon.kisti.re.kr), 한국의학논문데이터베이스(http://kmbase.medric.or.kr), 한국학술정보(http://kiss.kstudy.com), 한국교육학술정보원 학술연구정보서비스(http://www.riss.kr), 한국학술지인용색인(https://www.kci.go.kr), 전통의학 정보포털(https://oasis.kiom.re.kr)을 이용하였다. 문헌 검색 시 연도 제한 없이 2022년 7월 8일 검색일 이전의 모든 논문을 대상으로 하였다. 검색어는 “뇌졸중”, “중풍”, “뇌경색”, “뇌허혈”, “뇌출혈”, “뇌내출혈”, “뇌실질내출혈”, “지주막하출혈”, “뇌혈관질환”, “뇌색전”, “뇌혈전” 과 “한방”, “한의” 또는 “후유증”을 조합하여 검색하였고, 각각의 키워드는 개별적으로 검색하지 않고 두 가지를 조합하여 사용하였다.
3. 선정 및 배제기준
검색된 문헌 중 컴퓨터단층영상(Computed tomography, CT), 자기공명영상(Magnetic resonance imaging, MRI)을 이용하여 뇌졸중을 진단하였거나 뇌경색 혹은 뇌출혈로 진단명을 밝힌 문헌 중 인간 대상 연구로 한정하였으며, 한의 치료 중재의 효과에 대해 탐색한 임상 연구 중 부전마비, 완전마비, 강직, 운동실조 등 뇌졸중 후 운동 관련 후유증을 가진 뇌졸중 최초 발병자를 대상으로 하는 조건을 모두 만족하는 연구만을 선정하였다. 호소하는 증상에 대한 평가척도 중 추적 관찰을 위해 지속적으로 평가한 항목이 있는 연구만을 포함하였으며, 연구 디자인은 제한하지 않았다.
검색된 문헌 중 뇌졸중과 관련되지 않으며, 연구 논문이 아닌 기사, 잡지, 보고서 등의 간행물, 초록과 원문이 없어 내용을 검토할 수 없는 경우, 임상 연구가 아닌 문헌 고찰, 인체 유래물 연구, 뇌졸중 과거력이 있는 대상자가 포함된 연구, 발병일, 입원일, 혹은 치료 시작일을 밝히지 않거나, 그 기간을 밝히지 않아 실제 뇌졸중 시기를 알 수 없는 경우, 발병일부터 치료 시작까지의 기간을 평균과 표준편차로만 제시하고 최소 기간과 최대 기간을 확인할 수 없어 실제 뇌졸중 시기를 알 수 없는 경우, 서로 다른 뇌졸중 시기의 연구 대상자가 섞여 있는 경우, 근력, 가동범위, 기능 등 운동 평가척도가 포함되지 않거나 치료 후 지속 평가하지 않은 경우의 조건들 중 하나라도 해당하는 연구들은 배제하였다.
4. 자료의 추출 및 분석 방법
뇌졸중의 유형은 뇌경색(infarction)과 뇌출혈(hemorrhage)로 단순 분류하였으며, 뇌졸중 후유 증상은 상지와 하지 어느 한쪽이라도 Manual Muscle Testing(MMT)17,18 grade 0에서 1까지는 거의 움직임이 없는 상태로 보고 hemiplegia로, 상하지 모두 MMT grade 2 이상인 경우와 자각적 소력감을 호소하는 경우는 hemiparesis로 작성하였다.
중추성 뇌졸중 후 통증, 견관절 아탈구, 관절 구축, 강직 등 다양한 원인에 의하여 뇌졸중 후 통증이 동반된다. 시간이 지나도 이러한 통증이 호전되지 않은 경우, 강도는 더 강해지고 삶과 신체적 활동에 심각하게 영향을 주며19, 삶의 질(Quality of life, Qol)을 떨어뜨리고, 재활치료에 부정적 영향을 끼치게 된다20. 또 인지기능장애는 운동 능력 재습득과 보행을 방해하고 낙상 위험을 증가시키는 등 운동 회복에 큰 영향을 미친다21. 이러한 이유들로 근력의 저하, 어지럼증, 복시와 같이 보행 및 일상 생활 동작에 영향을 주는 증상 외에도 통증, 인지 저하, 우울감 등 운동 기능 회복에 직・간접적으로 부정적인 영향을 줄 수 있는 증상들도 분석에 포함하였다. 운동 장애와 운동 기능에 영향을 주는 증상을 평가하기 위해 활용된 평가척도는 1회만 평가한 경우라도 모두 포함하였으나 감각의 저하, 변비, 언어 장애 등은 운동 기능에 미치는 영향이 적을 것으로 판단되어 관련 증상 평가를 위해 평가척도를 사용하였어도 분석에 포함시키지 않았다.
1) 뇌졸중 시기의 분류
발병일로부터 치료 시작 시점까지의 기간을 확인하여 Berhardt 등2에서 정리한 기준에 따라 발병 후 7일 이내를 급성기, 발병 후 일주일부터 6개월까지를 아급성기, 6개월 이후를 만성기로 분류하여 30일을 한 달로 계산하여 뇌졸중 시기를 추정하였고, 각각의 논문에서 언급한 뇌졸중 시기를 함께 기록하였다. 시기를 언급하지 않은 경우를 밝히고, 실제 시기와 언급한 시기와의 일치도를 평가하였다.
American Physical Therapy Association에서 보고한 ‘stroke Evidence Database to Guide Effectiveness (EDGE)’ I과 II를 참고하여 보면, 뇌졸중 시기에 따라 평가척도의 활용 권고 정도가 다른 경우가 있었다22,23. 시기별 권고 수준이 달랐던 NIHSS, Berg Balance Scale(BBS)24,25, Functional Ambulation Categories(FAC)26,27, Functional Independence Measure (FIM)28, 36-Item Short Form Health Survey(SF-36)29를 포함하였고, 각각의 척도들은 뇌졸중 발병 후 2개월 미만, 2개월에서 6개월 사이, 6개월 이상 되는 시점을 기준으로 하여 평가되어 있었다. 이를 참조하여 척도별로 highly recommended 또는 recommended 수준으로 권고되고 있는 시기를 표시하였고, 포함된 연구들에서 평가척도가 실제로 사용된 시기를 표시하여 비교하였다.
2) 평가척도의 범주화
논문에서 사용된 평가척도들은 목적성에 따라 International Classification of Functioning(ICF) Category22를 일부 참고하여 분류하였다. ICF에서 ‘body function and structure’는 심리적 측면을 포함한 신체 전반 시스템의 생리적 기능과 신체의 해부학적 구조물들에서 일어난 손상을 평가하기 위한 척도들이 포함되어 있었다. 본 연구에서는 이 들 중 신체기능에 해당하는 부분들만 참고하여 기능(Function) 평가척도로 분류하였고, 나머지 인지와 심리 기능과 관련된 평가척도와 국소 해부학적 영역에서의 움직임과 관련된 평가척도는 임의로 세분화하여 분류하였다. ICF에서 일정한 작업 수행을 시행하려 할 때 주어지는 활동의 제한을 평가하기 위한 척도들은 ‘activity’로 분류되어 있었으며, 본 연구에서도 동일하게 적용하였다. ICF에서 ‘participation’으로 분류된 경우는 삶의 특정 상황에서의 참여와 관련된 평가척도들로, 본 연구에서는 삶의 질(Quality of life) 평가척도로 분류하였다. 그 외 주관적 증상의 정도를 정량화한 평가와, 보행에 대해 평가에 대하여 자체적으로 만든 기준을 사용한 경우는 임의척도(Self-measurement)로 분류하였고, 평가목적으로 사용된 의료기기(Medical device)도 따로 분류하였다.
3) 뇌졸중 한의 치료 핵심 지표 세트
핵심 지표 세트(Core Outcome Set, COS)는 연구자가 치료 중재의 효과를 입증하기 위해 특정 분야에 대한 연구를 수행할 경우 최소한으로 보고해야 하는 핵심 지표 세트로 전문가들이 권고한 평가척도의 목록이다30. 차 등31이 Conclusion of for the Korean Medicine Core Outcome Set for Stroke Sequelae(COS-SS-KM)로 정리한 modified Measure Yourself Medical Outcome Profile 2(mMYMOP2)32-34, aspartate transaminase(AST), alanine transaminase (ALT), blood urea nitrogen(BUN), creatinine(Cr), Five-level EuroQol-5 dimensions(EQ-5D-5L)35, EuroQol-Visual Analog Scale(EQ-VAS)36, Treatment satisfaction의 8가지 평가 항목을 기준으로 하여 포함된 논문 중 타 중재 치료 중 한약 치료가 복합 한의 치료의 일부로 포함된 경우는 배제하였고, 한약 치료 중재를 밝힌 연구만을 선별하여 활용도를 분석하였다.
III. 결 과
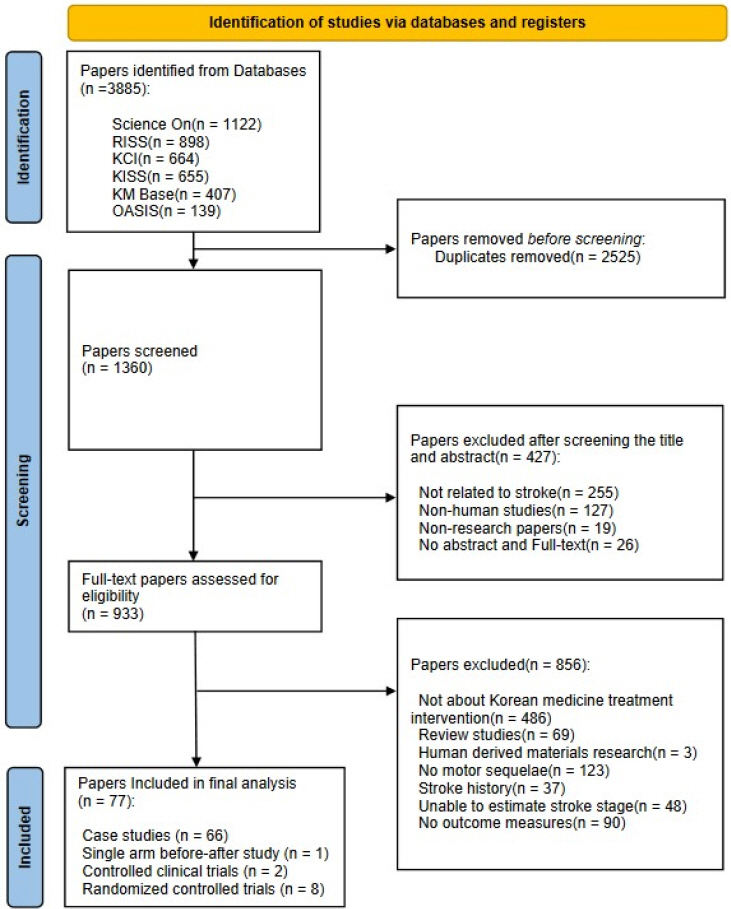
1. 문헌 선별
2. 일반적 특성과 시기 분류
임상 논문으로 증례 보고(Case report), 증례군 연구(Case series), 전향적 단일군 임상연구(Single arm before-after trial), 전향적 대조군 임상연구(Controlled clinical trial, CCT), 무작위 대조군 임상연구(Randomized controlled trial, RCT)가 포함되었다. 전체 중 증례 연구가 66편37,41-49,52-58,60-79,81-93,97,99-113으로 86%를 차지하였고, 다음으로 무작위 대조군 임상연구가 8편38,39,50,51,94-96,98으로 10%, 전향적 대조군 임상연구가 2편40,59으로 3%, 전향적 단일군 임상연구가 1편80으로 1%를 차지하였다.
연구 대상자의 증상은 부전마비, 완전마비, 운동실조, 보행장애, 의식저하, 어지럼증, 복시, 부종, 통증, 강직, 인지 저하, 우울감 등이 있었다.
대부분의 논문에서 뇌졸중 시기를 언급하지 않았고, 시기를 언급한 논문은 11편39,45,46,52,65,70,75,77,80,84,108이 있었는데, 그 중 2편45,52은 실제 시기와 언급된 시기가 일치하지 않았다. 송 등45은 뇌졸중 발병 후 2주 넘은 아급성기 단계의 환자 증례였는데, 제목과 본문에서 ‘급성 뇌경색 환자’로 기술하였으며, 김 등52은 뇌졸중 발병 후 19일 되는 시점에 입원하고 일반적인 재활치료를 하다가 호전이 되지 않아 1개월이 넘은 아급성기 단계에서 팔사혈(EX-UE9) 전침치료를 시행하여 수부 운동 장애에 효과를 본 증례 연구였으나 본문 중 환자를 ‘만성기 환자’로 기술하였다. 그 외 전향적 대조군 임상연구와 무작위 대조군 임상연구에서는 뇌졸중 시기를 언급한 경우가 급성기 환자를 대상으로 한 연구 1편39이었다. 시기별로는 아급성기 대상자 연구가 55편37,40-53,56,58-64,67-69,71-74,76,79,82,83,85,87,88,90-95,97-99,101,104-107,109,111-113으로 가장 큰 비중을 차지하였고, 급성기 대상자 연구가 16편38,39,54,55,57,65,70,75,77,81,96,100,102,103,108,110, 만성기 대상자 연구가 6편66,78,80,84,86,89으로 포함된 논문의 8%만을 차지하였다. 증례 연구에서는 아급성기 대상자 연구가 48편37,41-49,52,53,56,58,60-64,67-69,71-74,76,79,82,83,85,87,88,90-93,97,99,101,104-107,109,111-113으로 가장 많았고, 급성기 대상자 연구가 13편54,55,57,65,70,75,77,81,100,102,103,108,110, 만성기 대상자 연구가 5편66,78,84,86,89이었고, 전향적 단일군 연구 1편80은 만성기 대상 연구였으며, 대조군 임상연구에서는 만성기 대상자 연구는 한 편도 없었으며, 급성기 대상자 연구가 3편38,39,96, 아급성기 대상자 연구가 7편40,50,51,59,94,95,98있었다(Table 1, 2, Fig. 2).
Table 1
General Characteristics and Stroke Stage Classification of Case Studies (N=67)
| First author, year | Stroke type | Stroke lesion | Sample size | Symptoms | Intervention | Time since stroke | Real stroke stage | Described stroke stage | Consistency |
|---|---|---|---|---|---|---|---|---|---|
| Lee, 2000(a)64 | Hrr† | Rt.BG | 1 | Lt.hemiparesis, Dizziness | HM∥ | 1 w 5 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Lee, 2000(b)65 | Hrr† | Lt.frontal lobe deep white matter | 1 | Rt.hemiparesis, RUQ pain, LBP | HM∥, AT¶, MT**, cupping, WT†† | 1 d | acute | acute | C††† |
|
|
|||||||||
| Han, 200097 | Hrr† | ND§ | 1 | Lt.hemiplegia | ND§ | 2 m | subacute | ND§ | UE*** |
|
|
|||||||||
| Ko, 2000108 | Inf‡ | Lt.BG | 1 |
Rt.hemiplegia, Both malleolar edema, Consciousness disorder |
HM∥, AT¶ | 1 d | acute | acute | C††† |
|
|
|||||||||
| Lee, 200154 | Inf‡ |
Lt.BG & Rt.frontal lobe |
1 | Rt.hemiplegia, Tibia edema, Visual disturbance | HM∥, AT¶, PT‡‡, WT†† | 2 d | acute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2001(a)55 | Inf‡& Hrr† | Lt.MCA | 1 |
Rt.hemiparesis, Rt.flank pain, Dizziness, Edema |
HM∥, WT†† | 2 d | acute | ND§ | UE*** |
|
|
|||||||||
| Jeong, 200172 | Inf‡ | Lt.MCA | 1 |
Rt.hemiplegia, Consciousness disorder |
HM∥, AT¶, PT‡‡, WT†† | 3 w 1 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2001(b)79 | Hrr† | Both Cbll & ventricle | 1 |
Dizziness, Diplopia, Gait disturbance, uadriparesis |
HM∥, AT¶, WT†† | 1 m 5 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Lim, 200241 | Inf‡ | Midbrain & pons | 1 |
Rt.hemiplegia, Consciousness disorder |
HM∥, AT¶, PT‡‡, WT†† | 4 m 4 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kwack, 200266 | Hrr† | Rt.BG | 1 | Lt.hemiplelgia, Lt.spasticity | HM∥, AT¶, MT**, cupping, WT†† | >1 y 2 m | chronic | ND§ | UE*** |
|
|
|||||||||
| Kim, 200269 | Hrr† | Rt.BG | 1 | Lt.hemiparesis | HM∥, WT†† | 2 m 4 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Jang, 200276 | Inf‡ | Cbll | 1 | Ataxia, Dizziness | HM∥, AT¶, PT‡‡ | 1 w 4 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2003(a)70 | Inf‡ | Rt.MCA | 1 | Lt.hemiparesis, Dizziness | HM∥, AT¶, MT**, cupping, WT†† | 3 d | acute | acute | C††† |
|
|
|||||||||
| Lee, 200381 | Hrr† | Lt.thalamus | 1 |
Rt.hemiplegia, Dizziness, RUQ pain, Tremor |
HM∥, AT¶, PAT§§, PT‡‡, WT†† | 1 d | acute | ND§ | UE*** |
|
|
|||||||||
| Shin, 2003100 | Inf‡ | Lt.MCA | 1 | Rt.hemiparesis, Consciousness disorder | HM∥, AT¶, PT‡‡, WT†† | 1 d | acute | ND§ | UE*** |
|
|
|||||||||
| Jung,2003110 | Hrr† | Lt.BG | 1 | Rt.hemiparesis | HM∥, AT¶, WT†† | 1 d | acute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2003(b)111 | Inf‡ | Cbll | 1 | Vertigo, Ataxia | HM∥, AT¶, MT**, WT†† | 1 w 3 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Lee, 2004112 | Inf‡ | Lt.MCA | 1 | Rt.hemiplegia, Consciousness disorder | HM∥, AT¶, PAT§§, PT‡‡, WT††, aroma, taping | 1 m 15 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Lee, 200542 | Inf‡ |
Lt.Cbll & Lt.ganglia & PVWM |
1 | Rt.hemiparesis | HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | 2 w 3 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Ryu, 200549 | Inf‡ | Rt.MCA | 1 | Lt.hemiataxia, Chest pain, Dizziness | HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | 2 w 2 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Yoon, 200567 | Inf‡ | Lt.IC | 1 | Rt.hemiparesis | HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | 2 w 2 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Song, 200645 | Inf‡ | Lt.BG | 1 | Rt.hemiparesis, Depression, Dizziness | HM∥, AT¶, PT‡‡, WT†† | 2 w 2 d | subacute | acute | IC‡‡‡ |
|
|
|||||||||
| Woo, 200653 | Inf‡ | Lt.MCA | 1 | Rt.hemiplegia, Both knee pain | HM∥, AT¶, WT†† | 2 m 9 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Na, 200657 | Inf‡ | ND§ | 1 | Rt.hemiplegia | HM∥, AT¶, MT**, PT‡‡ | 6 d | acute | ND§ | UE*** |
|
|
|||||||||
| Hwang, 200778 | Inf‡ |
Lt.Cbll & Lt.Lateral medulla & both occipito-parietal lobes |
1 | Tremor, Spasticity, Dizziness | HM∥, AT¶, MT**, WT†† | 7 m 4 d | chronic | ND§ | UE*** |
|
|
|||||||||
| Yun, 2007102 | Inf‡ | Rt.MCA | 1 | Lt.hemiplegia | HM∥, AT¶, PT‡‡, WT†† | 3 d | acute | ND§ | UE*** |
|
|
|||||||||
| Goo, 200877 | Inf‡ | Cbll | 1 | Vertigo, Ataxia, Lt.hemiparesis, Diplopia, Nystagmus | HM∥, AT¶, cupping, WT†† | 1 d | acute | acute | C††† |
|
|
|||||||||
| Choi, 200887 | Inf‡ | Rt.Cbll | 1 | Ataxia, Vertigo | HM∥, AT¶, cupping, WT†† | 3 w 1 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 201156 | Inf‡ | ND§ | 1 | Rt.hemiplegia, Back stiffness | HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | 3 m 19 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Ryu, 201275 | Inf‡ | Lt.MCA | 1 |
Rt.hemiplegia, Depression, Both extremity rigidity |
HM∥, AT¶, MT**, WT†† | 6 d | acute | acute | C††† |
|
|
|||||||||
| Lee, 201437 | Inf‡ | Lt. thalamus | 1 | Rt.hemiataxia | HM∥, AT¶, MT**, WT†† | 1 w 3 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2014(a)71 | Inf‡ | Lt.thalamus | 1 |
Rt.hyperpathia, Rt.hemiparesis, Orthostatic dizziness |
HM∥, AT¶, PAT§§, PT‡‡, WT†† |
1 w 5 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2016(a)43 | Hrr† | Rt.pons | 1 | Lt.weakness, Dizziness, Diplopia, Ataxia | HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | 2 m 15 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Hwang, 201673 | Inf‡ | Rt.MCA | 1 |
Lt.hemiplegia, Edema, General weakness |
HM∥, AT¶, MT**, PT‡‡, WT†† |
2 m 5 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2016(b)83 | Inf‡ | Lt.MCA | 1 | Apraxia, Rt.hemiparesis |
HM∥, AT¶, MT**, PT‡‡, WT†† |
1 w 6 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Hong, 201690 | Inf‡ | Lt.ACA | 1 | Akinetic mutism, Rt.hemiplegia | HM∥, AT¶, WT†† | 2 w | subacute | ND§ | UE*** |
|
|
|||||||||
| Yang, 2016106 | Inf‡ & Hrr† |
Lt.ACA & Lt.parietal lobe |
1 | Rt.hemiplegia |
HM∥, AT¶, MT**, PT‡‡, WT†† |
2 w 4 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Seo, 2017113 | Inf‡ | Rt.MCA | 1 | Lt.hemiparesis, Lt.shoulder pain |
HM∥, AT¶, MT**, PT‡‡, WT†† |
4 m 19 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Cho, 201782 | Inf‡ | Lt.Cbll | 1 |
Dizziness, Gait disturbance, Ataxia, Lt.hemiparesis |
HM∥, AT¶, MT**, WT†† | 1 m 2 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Lim, 201786 | Hrr† | Lt.thalamus | 1 |
Rt.hyperpathia, Rt.hemiparesis, Gait disturbance, Rt. shoulder pain |
HM∥, AT¶, PAT§§, cupping, PT‡‡, WT†† | >6 m 19 d | chronic | ND§ | UE*** |
|
|
|||||||||
| Kim, 201789 | Inf‡ | Lt.BG | 1 | Rt.hemiparesis, Gait dusturbance | HM∥, AT¶, PT‡‡, WT†† | >2 y 11 m | chronic | ND§ | UE*** |
|
|
|||||||||
| Lee, 2017101 | Inf‡ | Rt.Cbll | 1 | Rt.hemiparesis, Gait disturbance, Dizziness, Diplopia | HM∥, AT¶, PT‡‡ | 1 m 13 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2018(a)46 | Inf‡ | Lt.BG | 1 | Rt.hemiparesis | HM∥, AT¶, PT‡‡, WT†† | 1 w 5 d | subacute | subacute | UE*** |
|
|
|||||||||
| Jeong, 201847 | Hrr† | Lt.BG | 1 | Rt.hemiparesis, Gait dusturbance |
HM∥, AT¶, MT**, PT‡‡, WT†† |
1 w 5 d | subacute | ND§ | C††† |
|
|
|||||||||
| Kim, 2018(b)52 | Inf‡ | Rt.BG & CR | 1 | Lt.hemiparesis | HM∥, AT¶, PT‡‡, WT†† | 1 m 5 d | subacute | chronic | UE*** |
|
|
|||||||||
| Seo, 201874 | Hrr† | Rt.BG | 1 |
Lt.hemiplegia, Cognitive disorder, Depression, General weakness |
HM∥, AT¶, WT†† | 3 m 3 d | subacute | ND§ | IC‡‡‡ |
|
|
|||||||||
| Kim, 2018(c)109 | Inf‡ & Hrr† | Lt.PICA | 1 | Vertigo, Ataxia |
HM∥, AT¶, MT**, PT‡‡ |
1 m 5 d | subacute | ND§ | UE*** |
|
|
|||||||||
| An, 201958 | Hrr† | Rt.BG & Ventricle | 1 | Quadriparesis, Consciousness disorder, Edema | HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | 3 m 12 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Chae, 201984 | Hrr† |
Lt.striatocapsular area & Frontal lobe & paracentral area & insula & temporal lobe |
1 | Rt.hemiplaresis, Gait disturbance | HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | >1 y 5 m | chronic | chronic | UE*** |
|
|
|||||||||
| Nam, 201985 | Inf‡ | Lt.Cbll & medulla | 1 | Ataxia, Dizziness | HM∥, AT¶, WT†† | 3 w 2 d | subacute | ND§ | C††† |
|
|
|||||||||
| Je, 201992 | Inf‡ & Hrr† |
Rt.MCA & Rt.frontal lobe |
1 | Lt.hemiparesis | HM∥, AT¶, WT†† | 2 w | subacute | ND§ | UE*** |
|
|
|||||||||
| Choi, 202063 | Hrr† | Lt.BG | 1 | Rt.hemiplegia, Gait disturbance, Rt. U/E pain |
HM∥, AT¶ (EA∥∥), PAT§§, taping, PT‡‡, WT†† |
2 m 21 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Bae, 202068 | Inf‡ | Cbll | 1 | Vertigo, Ataxia | HM∥, AT¶, PT‡‡ | 1 w 6 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Yang, 202091 | Hrr† | Rt.BG | 1 | Lt.hemiparesis, Gait disturbance |
HM∥, AT¶, MT**, PT‡‡, WT†† |
3 m 28 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Chae, 2020104 | Inf‡ | Lt.thalamus | 1 | Rt.hemiparesis, Gait disturbance | HM∥, AT¶, MT**, cupping, PT‡‡, WT††, FCST¶¶ | 3 w 5 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2020107 | Inf‡ | Lt.MCA | 1 |
Rt.hemiparesis, Gait disturbance, Cognitive disorder |
HM∥, AT¶, PT‡‡, WT†† | 2 w 1 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Jung, 202148 | Hrr† | Rt.BG & CR | 1 | Lt.hemiparesis | HM∥, AT¶, cupping, MT**, PT‡‡, WT†† | 2 w 1 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Chae, 202193 | Inf‡ | Rt.MCA | 1 | Lt.hemiparesis, Gait disturbance | HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | 3 w 5 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Yang, 2022105 | Inf‡ | Rt.BG | 1 | Lt.hemiplegia, Gait disturbance | HM∥, AT¶, MT**, PT‡‡, WT†† | 1 m 25 d | subacute | ND§ | UE*** |
|
|
|||||||||
| Jeon, 200288 |
1) Hrr† 2) Hrr† |
1) subarachnoid & Lt.subcortex -putaminal area 2) Lt.putaminal area |
2 | Rt.hemiplegia | HM∥, AT¶, MT**, PT‡‡, WT†† |
1) 2 w 6 d 2) 1 w 5 d |
subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2004103 |
1) Inf‡ & Hrr† 2) Inf‡ & Hrr† |
1) Lt.BG & BothPVWM 2) Rt.MCA & Rt.parietallobe |
2 |
1) Rt.hemiparesis, Consciousness disorder 2) Lt.hemiparesis, Dizziness, Consciousness disorder |
HM∥, AT¶, MT**, cupping, PT‡‡, WT†† | 1) 1 d 2) 1 d | acute | ND§ | UE*** |
|
|
|||||||||
| Choi, 200662 |
1) Hrr† 2) Inf‡ |
1) Rt.thalamus 2) Lt.MCA & Lt.PCA |
2 |
1) Lt.hemiparesis, Lt. foot drop, Knee pain, Back pain, Lt. shoulder pain 2) Rt.hemiparesis, Rt. Foot drop, Lt. shoulder pain |
HM∥, AT¶, MT**, taping, PT‡‡, WT†† |
1) 3 w 4 d 2) 4 m 6 d |
subacute | ND§ | UE*** |
|
|
|||||||||
| Shin, 200699 |
1) Hrr† 2) Inf‡ 3) Inf‡ |
1) Rt.BG 2) ND§ 3) Rt.MCA |
3 |
1) Lt. shoulder pain, Lt.hemiplegia 2) Rt. shoulder pain, Rt.hemiparesis 3) Lt. shoulder pain, Lt.hemiplegia |
HM∥, AT¶, cupping, PT‡‡, WT†† |
1) 3 m 18 d 2) 4 w 3) 2 m 16 d |
subacute | ND§ | UE*** |
|
|
|||||||||
| Han, 200861 |
1) Hrr† 2) Hrr† |
1) Lt.LN & Lt.PVWM 2) Lt.BG |
2 |
1) Rt.hemiplegia, Gait disturbance, Rt. hand edema, Rt. Shoulder pain 2) Rt.hemiplegia, Rt. Shoulder pain, Gait disturbance |
AT¶, PAT§§ |
1) 1 m 3 d 2) 1 m 21 d |
subacute | ND§ | UE*** |
|
|
|||||||||
| Kim, 2014(b)44 |
1) Hrr† 2) Hrr† 3) Hrr† |
1) Rt.BG 2) Lt.thalamus 3) pons |
3 |
1) Lt.hemiparesis 2) Rt.hemiparesis 3) Lt.hemiparesis, Dizziness |
HM∥, AT¶, PT‡‡ |
1) 2 w 6 d 2) 1 w 5 d 3) 1 m 12 d |
subacute | ND§ | UE*** |
|
|
|||||||||
| Byun, 201460 | Inf‡ |
1) Rt.MCA 2) Lt.MCA 3) Rt.MCA |
3 |
1) Lt.hemiparesis, Lt. U/E pain 2) Rt.hemiparesis, Rt. U/E pain 3) Lt.hemiparesis, Lt. U/E pain |
HM∥, AT¶, PAT§§, PT‡‡, WT†† |
1) 1 m 8 d 2) 2 m 4 d 3) 1 m 9 d |
subacute | ND§ | UE*** |
|
|
|||||||||
| Baek*, 201480 | Inf‡ or Hrr† | ND§ | 7 | Hemiplegia, U/E spasticity | AT¶ | ≥6 m | chronic | chronic | C††† |
* Single arm before-after trial, †Hrr : hemorrhage, ‡Inf : infarction, §ND : not described, ∥HM : herbal medicine, ¶AT : acupuncture,
Table 2
General Characteristics and Stroke Stage Classification of Controlled Trials (N=10)
| First author, year | Study design | Intervention | Stroke type | Stroke lesion | Symptoms | Time since stroke | Real stroke stage | Described stroke stage | Consistency | |
|---|---|---|---|---|---|---|---|---|---|---|
|
|
||||||||||
| Test (sample size) | Control (sample size) | |||||||||
| Sim, 200440 | CCT* | A : Chuna+B (n=21) | B : AT‡, WT§ (n=19) | Inf§§ | ND¶¶ | Hemiplegia, U/E spasticity | ≥3 w (25~112 d) | subacute | ND¶¶ | UE*** |
|
|
||||||||||
| Chang, 200459 | CCT* | A : MT∥+B (n=35) | B : AT‡, PT¶, WT§ (n=33) | Inf§§ or Hrr∥∥ | ND¶¶ | Hemiparesis | 10~30 d | subacute | ND¶¶ | UE*** |
|
|
||||||||||
| Seo, 2001(a)38 | RCT† | A : AT‡ (contralateral)(n=6) | B : AT‡ (ipsilateral) (n=7) | Inf§§ or Hrr∥∥ | BG/MCA/ PVWM/pons | Hemiparesis | ≤1 w | acute | ND¶¶ | UE*** |
|
|
||||||||||
| Seo, 2001(b)39 | RCT† | A : AT‡ (contralateral)(n=6) | B : AT‡ (ipsilateral) (n=7) | Inf§§ or Hrr∥∥ | BG/MCA/ PVWM/pons | Hemiparesis | ≤1 w | acute | acute | C††† |
|
|
||||||||||
| Sim, 200394 | RCT† | A : HM**, AT‡ (Yin meridian EA‡‡), PT¶, WT§(n=27) | B : HM**, AT‡ (Yang meridian EA‡‡), PT¶, WT§(n=26) | Inf§§ or Hrr∥∥ | ND¶¶ | Hemiplegia, U/E spasticity | 2 w~5 m (17~140 d) | subacute | ND¶¶ | UE*** |
|
|
||||||||||
| Choi, 200398 | RCT† | A : MT∥+B (n=20) | B : HM**, AT‡, PT¶ (n=20) | Inf§§ | MCA | Hemiplegia | ≥2 w ≤5 w | subacute | ND¶¶ | UE*** |
|
|
||||||||||
| Cho, 200595 | RCT† | A : HM**, AT‡, PT¶, WT§, PAT†† (Zingiberis Rhizoma) (n=12) | B : HM**, AT‡, PT¶, WT§, PAT†† (Bee venom) (n=11) | Inf§§ or Hrr∥∥ | ND¶¶ | Hemiplegia, Shoulder pain | 3 w~2 m (25~51 d) | subacute | ND¶¶ | UE*** |
|
|
||||||||||
| Hong, 200650 | RCT† | A : HM**, AT‡ (2 Hz EA‡‡), PT¶, WT§ (n=21) | B : HM**, AT‡ (120 Hz EA‡‡), PT¶, WT§ (n=21) | Inf§§ | Motor cortex/ CR/IC/ Brain stem | Motor dysfunction | 1 w~1 m | subacute | ND¶¶ | UE*** |
|
|
||||||||||
| Kim, 200751 | RCT† | A : HM**, AT‡ (2 Hz EA‡‡), PT¶, WT§ (n=32) | B : HM**, AT‡ (120 Hz EA‡‡), PT¶, WT§ (n=30) | Inf§§ | ND¶¶ | Motor dysfunction | 1 w~1 m | subacute | ND¶¶ | UE*** |
|
|
||||||||||
| Kim, 200896 | RCT† | A : AT‡ (EX-UE9) +B (n=31) | B : HM**, AT‡, MT∥, PT¶ (n=31) | Inf§§ or Hrr∥∥ | Crb/Cbll/ midbrain/ pons | Hemiparesis | ≤1 w | acute | ND¶¶ | UE*** |
* CCT : controlled clinical trial, †RCT : randomized controlled trial, ‡AT : acupuncture, §WT : Western medicine treatment, ∥MT : moxibustion, ¶PT : physical therapy,

3. 평가척도의 활용도 및 시기 적절성에 관한 분석
기능(Function) 평가척도는 5가지가 사용되었고, 그 중 NIHSS가 11회로 가장 많이 활용되었다. 활동(Activity) 평가척도는 14가지로 다양하게 사용되었으며, 그 중 Modified Barthel Index(MBI)114가 27회로 가장 많이 활용되었다. 가동(Motion) 평가척도는 5가지가 사용되었고 MMT가 55회로 가장 많이 활용되었다. 삶의 질(Quality of life) 평가척도는 SF-36와 Dizziness Handicap Inventotry(DHI)115 2가지가 사용되었다. 인지상태 평가척도로는 MMSE가 6회 사용되었다. 임의척도(Self-measurement)는 전체 중 3번째로 많이 사용되었고, 보행의 단계, 어지러움의 정도, 통증의 정도, 진전의 정도, 부종의 정도 등이 평가되었다. Visual Analogue Scale(VAS)116과 Numeric Rating Scale(NRS)116은 각각 9회씩 사용되었으며, 어지러움, 통증, 복시 등이 평가되었다. 의료기기 중 뇌졸중 후 동반되는 마비 측의 어깨 통증을 평가 하기 위하여 X-ray를 사용한 경우는 1회에 불과했다(Table 3).
Table 3
Outcome Measurement of Included Studies (N=77)
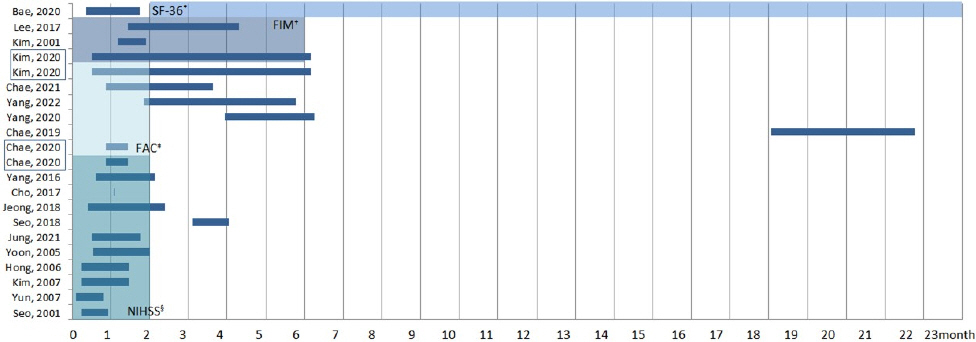
NIHSS는 뇌졸중 후 신경학적 결손을 측정하기 위한 정량적 도구로, 2개월을 넘어선 아급성기와 만성기에서는 더 이상 권고되지 않는 것으로 보고 되어있으나, 3개월이 넘은 시점에서 사용한 논문이 1편74 있었고, 발병 후 32일 된 시점에서 초진 평가만 시행하고 치료 후에 평가하지 않은 논문도 1편82 있었다. FAC는 뇌졸중 발병 후 2개월 이내에 평가하도록 권고하고 있으나, 6편84,91,93,104,105,107의 논문 중 4편93,104,105,107은 권고 기간 내에 처음 평가되었고, 그 중 1편104 만이 권고 기간 내에 최종 평가되었으며, 2편84,91은 처음 평가와 최종 평가 모두 권고 기간 내에 평가되지 않고 3개월을 넘어서 평가되거나, 1년 6개월이 넘은 상황에서 평가되었다. FIM은 뇌졸중 발병 후 6개월까지는 높은 수준으로 권고되고 있으며 3편79,101,107의 논문 모두 시기 적절하게 사용되었다. SF-36는 뇌졸중 발병 후 2개월을 넘어선 아급성기와 만성기에 권고되고 있으나, 사용된 1편68의 논문에서 발병 후 11일과 2개월 이전에 두 차례 평가하여 권고 기간에서는 벗어나 있었음을 확인할 수 있었다68(Fig. 3).
Fig. 3
Timeliness of the applied clinical outcome variables (N=19).
The shade of the background means the appropriate phase to apply the outcome. Studies grouped in boxes are identical studies.
*SF-36 : 36-Item short form health survey, †FIM : functional independence measure, ‡FAC : functional ambulation categories, §NIHSS : national institutes of health stroke scale
추가로 BBS는 뇌졸중 시기와 관계없이 활용할 수 있어 Fig. 3에 표시되어 있지는 않으나, strokEDGE에 따르면 2개월이 지난 아급성기와 만성기에 보다 더 높은 수준으로 권고되고 있으며, 1편43만이 2개월을 초과한 시기에 사용하였고 나머지 4편44,85,87,101은 2개월 이전에 사용하였다. 또 MMSE는 strokEDGE I과 II에서 제시되지는 않았으나, Nys 등10에 의해 수행된 선행 연구에 따르면 2주 이내 뇌졸중 후 인지 영역 손상에서는 치매보다 복합적인 인지기능의 손상이 나타나므로, 선별도구로 사용 시 평가 결과에 대하여 해석에 주의해야 한다고 하였다. 그러나 본 연구에 포함된 논문 양 등106, 조 등82, 이 등101, 정 등47, 김 등107, 정 등48 6편 중 1편47은 발병 후 12일이 된 시점에서 평가되었다.
4. 핵심 결과 지표의 활용
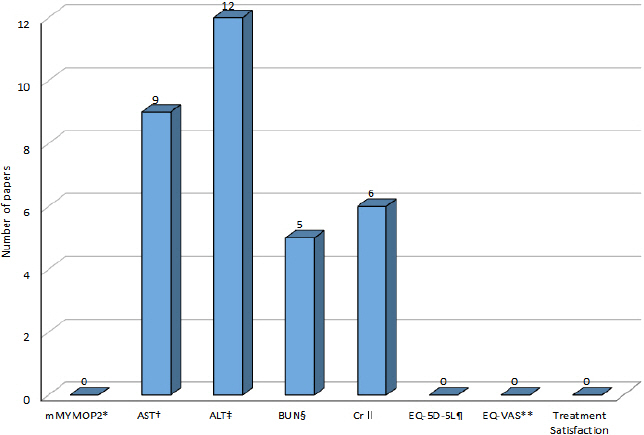
한약 치료 중재를 밝힌 연구 63편37,41-49,52-58,60,62-79, 81-87,89-93,99-113에 한하여 차 등31의 연구를 바탕으로 COS-SS-KM의 8가지의 핵심 지표의 활용도를 확인 해본 결과, 단 17편37,41,44,46,54,55,57,58,65,71-73,77,81,100,111,112만이 제시된 평가 지표 중 사용된 항목이 있었으며, 17편 모두 증례 연구에서 입원기본검사를 목적으로 시행된 것으로서 AST, ALT, BUN, Cr가 제시되었다. 또한 간 기능 검사(Liver function test, LFT)로 AST와 ALT를 같이 쓴 경우는 9편41,55,57,65,72,77,81,100,111, 신장 기능 검사(Renal function test, RFT)로 BUN과 Cr을 같이 쓴 경우는 4편54,55,73,100이었고, 4개 항목을 모두 다 같이 쓴 경우는 2편55,100뿐이었다. 그리고 이 중 추적 검사를 시행한 연구는 9편41,54,55,57,65,72,73,81,100이었다. 이 중 한약 치료에 대한 간 기능 및 신장 기능에 대한 안전성은 언급되지 않았다. 그리고 63편의 연구에서 mMYMOP2나 EQ-5D-5L, EQ-VAS, 그리고 치료 만족도 평가를 시행한 경우는 없었다(Fig. 4).
Fig. 4
Core outcome set utilization in herbal medicine clinical research (N=17).
*mMYMOP2 : modified measure yourself medical outcome profile 2, †AST : aspartate transaminase, ‡ALT : alanine transaminase, §BUN : blood urea nitrogen, ∥Cr : creatinine, ¶EQ-5D-5L : five-level EuroQol 5-demensions, **EQ-VAS : EuroQol visual analogue scale
IV. 고 찰
뇌졸중 환자 중 운동기능장애를 가진 경우를 대상자로 하는 국내 한의 임상 연구들을 분석하기 위하여 6개의 논문 데이터베이스를 이용하여 검색한 결과 77편의 논문을 선정하였다. 분석에 포함된 연구 대상자의 증상은 부전마비, 완전마비, 운동실조, 보행장애 등 운동 관련 후유증과 그에 영향을 주는 의식저하, 어지럼증, 복시, 부종, 통증, 강직, 인지 저하, 우울감 등이 있었다. 시간이 지남에 따라 환자는 더 복합적이고 전신적인 증상들을 겪기 때문에 시기별로 한・양방 치료 방법이 다르게 적용되고 있다. 치료 방법을 선정하거나, 치료 효과를 확인하거나, 예후를 판단하기 위해서뿐만 아니라, 임상 연구에서 결과의 해석과 지식 통합을 위한 하위 연구로 사용되기 위해서는 뇌졸중 시기를 확인할 수 있는 정보를 밝히고 시기에 부합한 평가척도를 활용하는 것이 중요하다. 그러나 국내 데이터베이스를 통하여 검색된 국내 뇌졸중 후유증 한의 임상 연구 77편을 분석한 결과, 뇌졸중 시기에 대해서 분명히 밝히지 않은 경우가 많았고, 시기별로 적절한 평가척도를 사용하지 못한 경우도 있었으며, 한의약 임상 연구에서 기본적으로 요구되는 평가척도 활용도 미흡하였다.
1. 뇌졸중 시기 보고 충실도
뇌졸중 재활치료를 위한 한국형 표준 진료 지침에 따르면 급성기 뇌졸중 환자의 재활치료는 내과적으로 안정이 되면 가능한 한 빠른 시간 내에 시작할 것을 권고하고 있다117. 이러한 결과는 뇌신경 가소성 원리에 따라 조기에 적극적으로 재활치료를 시행하는 경우 뇌졸중 후유증을 최소화할 수 있기 때문에 지속적으로 강조되어왔다118. 본 연구에서도 만성기 대상자 연구 대비 급성기와 아급성기 대상자 연구의 수가 많은 것을 확인할 수 있었다. 선정된 77편의 논문 중 시기를 밝혀 적은 경우는 11편에 불과하였으나, 시기를 언급한 경우에는 기준에 맞도록 적절하게 언급된 경우가 많았고, 단 2편에서 실제 시기와 언급된 시기가 일치하지 않았다. 특히, 시기를 언급한 논문은 11편 중 10편은 모두 증례 연구였으며, 대조군 임상연구에서는 단 한 편의 연구만이 뇌졸중 시기를 언급하고 있었다. 뇌졸중 시기는 급성기에서 아급성기로, 아급성기에서 만성기로 이행되어가는 연속적인 과정이지만, 뇌졸중 운동기능장애의 자연적 회복기와 정체기의 시기적 특성을 고려하였을 때 뇌졸중 시기에 대한 언급은 반드시 필요할 것으로 사료된다.
2. 사용된 평가척도와 시기별 적절성
임의 척도를 제외하고 포함된 연구들 중 가장 높은 빈도로 사용된 평가척도 3가지는 MMT, MBI, NIHSS였다. MMT는 근력과 근육의 기능을 측정하는 표준화된 척도로 1분 이내로 빠르게 검사할 수 있어 평가가 용이하기 때문에 임상과 연구에서 가장 흔히 사용되고 있다18. MBI는 기능적 독립성을 측정하는 도구로 Activities of daily living(ADL) 평가척도 중 임상과 연구에서 흔하게 사용되는 것으로 알려져 있다119. MBI는 환자에게 어떤 재활 치료가 적절할지에 대한 정보를 준다면, NIHSS는 뇌졸중 후 신경학적 결손을 측정하여 조기 예후 판정하는 지표로 유용하게 사용되고 있다120. 그래서 NIHSS는 발병 후 2개월 전으로만 권고되고 있으나, 서 등74에서는 3개월이 넘어서 사용하였고, 입원 시와 퇴원 시 측정 점수는 모두 9점으로 변화가 없었다. FAC는 물리치료를 받는 환자에서 기능적 이동성과 보행을 평가하는 도구로 뇌졸중 발병 후 2개월 전으로만 권고되고 있으나, 권고 기간에서 벗어나서 사용한 경우가 2편 있었다84,91. SF-36는 건강상태를 정량화하고 건강 관련 삶의 질(Health-related Qol)을 측정하는 도구로 뇌졸중 발병 후 2개월을 넘어선 아급성기와 만성기에 권고되나 SF-36을 사용했던 연구는 발병 후 11일이 된 시점에서와 34일이 된 시점에서 두 차례 평가한 것을 확인할 수 있다68. Ducan 등121의 선행 연구에 따르면 급성기 뇌졸중 임상연구에서 활용된 평가척도를 분석한 결과 평가척도 선정 및 평가의 시점에서 일관성을 보이지 않았던 점을 보고한 바 있었다. 따라서 뇌졸중 특이 평가척도를 사용하기 전에 앞서 연구 대상자의 발병일로부터의 시기를 고려하여 적절한 평가척도를 선정하여야 할 것이다. 추가로 뇌졸중 후 어깨 통증과 가동 범위 제한이 있는 경우 한 등61의 연구에서와 같이 X-ray를 활용하거나, 변 등60, 김 등71의 연구에서와 같이 Complex regional pain syndrome(CRPS), CPSP 에서 Digital Infrared Thermal Imaging(DITI)을 활용하거나, 백 등80의 연구에서와 같이 spasticity에서 탄성초음파 검사 기기를 활용하는 등 영상의학적 진단기기를 사용한 경우는 4편에 불과했으며 향후 연구에서 뇌졸중 통증과 강직과 관련하여 보다 적극적으로 영상의학적 진단 평가를 활용해야 할 것이다.
삶의 질 평가척도로는 DHI와 SF-36 두 가지가 있었으며, 배 등68의 연구에서 두 평가척도를 모두 사용하였다. 두 평가 모두 환자가 스스로 본인의 상태와 기분에 대하여 답변하여 보고하는 방식의 설문평가이며 DHI의 경우는 functional 부분 9개, emotional 부분 9개, physical 부분 7개 질문으로 구성되어 있고, 어지럼증으로 인하여 일상생활에서 스스로가 인식하고 있는 불편감을 적도록 한다. SF-36은 physical functioning, role limitations due to physical problems, general health perceptions, vitality, social functioning, role limitation due to emotional problems, general mental health, health transition 8개 부분을 평가한다. 그러나 뇌졸중 환자에서 조기 삶의 질 평가는 환자를 위한 더 나은 중재를 촉진하고 장애를 최소화하는 측면에서 중요하다고 보고된 바 있고122, 신체적, 정신적 건강이 뇌졸중 환자와 보호자 삶에 큰 영향을 주기에 더 나은 회복과 더 나은 삶을 위해 뇌졸중에서 건강 관련 삶의 질 평가가 중요하다고 보고된 바 있으나123, 본 연구에서 삶의 질 평가를 한 논문은 단 1편에 불과하여 향후 삶의 질 평가의 적극적 활용이 필요할 것으로 보인다. 추가적으로 임의 지표 보다는 객관적 평가척도를 사용하고, grade를 사용한 경우 참고한 척도를 반드시 적거나 명칭, 출처 등을 밝혀 적어야 할 것으로 보인다.
3. 핵심 평가척도와 한의약 안전성 보고 충실도
COS는 체계적 문헌 고찰이나 메타 분석의 형태로 여러 기존 연구의 결과를 비교 및 대조하고 결합 및 해석하는 과정에서 유용한 연구 성과를 내기 위한 측면에서 중요하다. 동일 치료 중재에서 서로 다른 평가척도를 사용하면 치료 효과에 대해 결정적인 권고가 어려워진다. 따라서 연구 전반에 걸쳐 결과 보고를 표준화하여 다양한 상황, 환경 및 사람에서 치료 중재의 효과를 더 잘 비교 및 대조할 수 있도록 하고, 최소한의 보고 지표를 둠으로써 결과 보고 편향 또는 출판 편향을 피할 수 있다124. 차 등31의 연구에 따르면 최종적으로 8개 평가 항목이 COS-SS-KM에 포함되었고, 본 연구 포함 논문 중 한약 치료 중재를 밝힌 논문 17편 중 COS-SS-KM 항목은 drug safety 측면에서 요구된 AST, ALT, BUN, Cr 4가지 항목만이 활용되었고, symptoms, Qol, satisfaction 측면에서의 항목들은 활용되지 않았다.
한약의 안전성에 대한 논란은 잔류농약과 중금속 등 약재의 오염과 관련된 문제와 함께, 한약 자체의 독성에 의한 간손상이나 신손상 등이 주로 제기되고 있는데,125 이에 따라 안 등125, 박 등126, 이 등127의 연구와 같이 한약 투여의 안전성을 입증하기 위한 연구가 보고된 바 있었고, 윤 등128은 한약 복용으로 인한 약인성 간손상 발생을 정확히 파악하고 예방을 위한 대책을 수립하기 위해서는 전향적인 연구 설계로 약인성 여부 판정에 필요한 항목을 빠짐없이 조사하고 보고할 필요가 있다고 주장하였다. 이렇듯 선행 연구를 통하여 LFT 및 RFT를 통한 한약 투여 안전성 검토의 필요성을 이미 인지하고 있었기 때문에, 연구에서 AST, ALT, BUN, Cr의 항목을 기록한 것은 이러한 노력이 반영된 것으로 사료된다. 그러나 17편의 논문은 모두 증례 연구였으며, 증례 연구는 입원 기본검사를 초진 평가에 그치거나, 정상 범위를 초과하는 경우에만 기록하고 있기 때문에, COS가 누락되었다고 일률적으로 평가하기는 어렵다. 다만, 향후 연구에서는 안전성과 관련되어 임상에서 평가가 이루어졌다면, COS 지표를 적극적으로 활용하는 것이 좀 더 충실한 정보를 제공할 수 있을 것으로 판단되며 이에 대해서는 추가적인 논의가 필요하다. 또한 김 등55은 한약 치료가 신기능 개선에 효과를 보인다고 하였고, 이 등65은 한약의 치료 효과와 안전성이 객관적으로 검증되지 못한 점을 주장하기는 하였으나, 한약 치료 후 우려한 바와 달리 뚜렷한 간기능 개선 효과를 나타내었다고 하였으며, 황 등73은 한약 투여가 사구체 여과율(estimated glomerular filtration rate, eGFR) 수치를 포함한 병리검사 상 신장기능을 악화시키지 않는다고 하였다. 하지만 3편의 논문 모두 안전성에 대한 언급이 명확하지는 않았다. 기존의 논문들은 차 등31의 연구가 발표된 2022년 이전 논문들이므로 반드시 해당 기준을 적용해야 한다고 말할 수는 없으나, 기존 논문들에서 이런 지표들의 보고가 부족한 현황이며 이 지표들을 보고함으로써 가지는 필요성으로 인하여 추후 연구에서는 적용이 필요하다.
4. 후속 연구의 제언
본 연구에서는 뇌졸중 후 운동기능장애에서 회복의 시기적 특성을 고려하여 논문에서 뇌졸중 시기와 관련된 정보를 위주로 추출하여 분석하였다. 향후 연구에서는 운동 관련 후유증 외에 언어기능이나 인지기능의 손상 후 회복에 있어서 시기적 특성에 대하여 분석하는 연구가 필요할 것으로 보인다. 또한, 본 연구에서는 평가의 시기적 측면을 살펴보았으므로, 후속 연구에서는 시기에 따른 치료 전략에 관한 분석 연구도 필요할 것으로 사료된다. 본 연구는 국내 뇌졸중 후유증 연구에서 뇌졸중 시기 보고의 필요성을 알렸다는 점과, 뇌졸중 시기별 평가 전략에 대해 제고하였다는 점에서 의의가 있다. 또한 뇌졸중 한의약 임상 혹은 연구 현장에서 기본 프로토콜로 자리 잡아야 할 핵심 평가 지표에 대해 상기시켰다는 데에 의의가 있다. 그러나 본 연구는 뇌졸중 한의 치료 임상 혹은 연구 현장에서 전반적으로 활용되는 평가척도와 연구 대상 자의 뇌졸중 시기 및 시기의 언급을 관찰하기 위하여 연구 디자인을 제한하지 않았지만, 결과적으로 선정된 문헌들의 대부분이 증례 연구라는 점에서 후속 연구에서는 연구 디자인을 구분하여 분석하는 연구가 필요할 것으로 보인다. 이에 향후 연구에서는 증례 보고를 배제하고 일정 기간 한약 투여를 중재로 시행한 뇌졸중 한의 임상 연구 논문들을 선별하여 핵심 평가 지표의 활용을 평가해보아야 보다 정확한 활용도를 분석해볼 수 있을 것으로 사료된다. 또한 본 연구는 평가척도 위주의 분석을 하여 개별 의료기기에 관하여서 다루지 못하였으므로 향후 관련 연구가 필요하다. 마지막으로 뇌졸중의 유병율이 연령이 증가함에 따라 높아진다는 특성129을 고려하여 문헌 선정 시 연구 대상 연령 기준을 두거나 연구에서 연령 정보를 추출하여 연령층별로 구분 지어 분석하지 못하였으므로 향후 보다 면밀한 연구 설계를 통하여 뇌졸중 한의 임상 연구를 다각도로 분석하는 연구가 필요하다.
V. 결 론
본 연구는 뇌졸중 후 운동 관련 후유증을 가진 환자를 대상으로 하는 국내 한의 임상 연구를 분석한 연구로 뇌졸중 시기 보고의 충실도, 평가 시기의 적절성 및 핵심 평가척도의 활용도에 대하여 보고한 연구이다. 연구 결과, 뇌졸중으로 인한 운동 관련 후유증을 대상으로 하는 국내 한의 임상 연구들에서 뇌졸중 시기 보고가 미흡하였으며, 급성기와 아급성기 위주의 연구로 시기적 편향성을 보였다. 또한, 핵심 평가척도의 활발한 활용이 이루어지지 않고 있었으며, 한의약 안전성에 대한 평가가 부족하였다. 후속 연구에서는 뇌졸중 시기를 충실히 보고해야 하고, 임상과 연구에 있어서 더 나은 치료 효과나 연구 성과를 위해 뇌졸중 시기에 따른 적절한 평가 지표를 선정하는 것이 필요하다. 또한, 뇌졸중 임상 연구 시 핵심 평가척도를 반영한 기본 프로토콜을 구성하고 연구에 한의약 안전성 보고도 포함하는 것이 필요하다.


