Yukgunja-tang for Irritable Bowel Syndrome: A Protocol for a Systematic Review and Meta-Analysis
Article information
Abstract
ABSTRACT
Background:
Irritable bowel syndrome (IBS) is a digestive disorder characterized by abdominal discomfort or pain accompanied by a change in stool condition. Owing to its complicated mechanisms, a standard treatment for IBS has not yet been established.
Yukgunja-tang (YGT) is a Korean herbal medicine known in Asia to be effective in the treatment of gastrointestinal symptoms. In this study, we will conduct a systematic review of randomized controlled trials (RCTs) to assess the efficacy and safety of YGT in IBS treatment.
Methods and analysis:
English databases, such as Embase, Medline (via PubMed), Allied and Complementary Medicine Database, and Cochrane Central Register of Controlled Trials, will be searched for articles published up to April 2023. Additional databases, such as five Korean, one Chinese, and one Japanese database, will be included. RCTs and quasi-RCTs will also be included in the assessment of the efficacy of YGT. The overall efficacy rate will be the primary outcome, and data such as IBS quality-of-life measurements, global symptom scores, and adverse events will be the secondary outcomes. Review Manager Version 5.3 will be used for evaluation, and the risk of bias (RoB) will be evaluated using Cochrane Collaboration’s RoB tool. The Grading of Recommendations Assessment, Development, and Evaluation approach will be used to score the quality of evidence.
Conclusion:
This study will demonstrate the efficacy and safety of YGT for treating patients with IBS.
I. Introduction
Irritable bowel syndrome (IBS) is a digestive disorder characterized by abdominal discomfort or pain accompanied by a change in stool condition without structural abnormalities1. Many patients’ quality of life is adversely affected because of recurrent symptoms2. The global prevalence of IBS was 9.2% in 2020 based on Rome III criteria3.
IBS seems to involve complicated mechanisms such as visceral hypersensitivity, abnormal motility, dietary intolerance, enhanced pain perception, autonomic nervous system abnormality, and neural and immunological communication4. Primary treatment for IBS is the use of medications such as loperamide, tricyclic antidepressants, rifaximin, and selective serotonin receptor inhibitors5. However, there are some limitations to their efficacy and side effects such as dry mouth6.
In Asia, herbal medicine has been used, which has fewer side effects than Western medicine7. Yukgunja-tang (YGT) is a traditional Korean herbal medicine (Rikkunshi-to in Japan and Liu-Jun-Zi-Tang in China) that is known to be effective in treating gastrointestinal symptoms in Asia8. Moreover, modified YGT (YGT added with specific herbs) can be used to treat gastric fullness and gastrointestinal symptoms9 which are similar to the clinical manifestations of IBS. YGT consists of Atractylodis lanceae rhizoma (5.63 g), Ginseng radix (3.75 g), Pinellia tubers (5.63 g), Poria cocos (3.75 g), Zizyphi fructus (3.75 g), Aurantii nobilis pericarpium (3.75 g), Glycyrrhizae radix (1.88 g), and Zingiberis rhizoma (3.75 g). Several studies using YGT reported the positive effect on functional gastrointestinal diseases8,10, however, there are still lack of studies on the use of YGT for IBS.
In this study, we will conduct a meta-analysis and systematic review of the efficacy and safety of YGT for IBS to provide evidence for using YGT as an alternative treatment for IBS.
II. Methods
1. Study registration
A protocol has been registered on PROSPERO (ID: CRD42023400078).
2. Inclusion criteria for study selection
1) Types of studies
This systematic review will include published randomized controlled trials (RCTs) and quasi-RCTs. Case studies, commentaries, and animal research will be excluded.
2) Types of patients
Patients who fulfilled the Rome diagnostic criteria, including age, sex, and race, will be included in this study. As the first Rome criteria standard was established in 199211, studies before 1992 will be screened, and similar criteria (e.g., Manning and Kruis criteria)12 will be included with agreement among researchers. Studies on IBS patients with other diseases, such as inflammatory bowel disease or colorectal cancer, will be excluded.
3) Types of interventions
Studies using YGT and modified YGT for IBS treatment will be included. The comparator groups will be conventional Western medicine, placebos with the same appearance and odor as YGT, and the waiting group with no treatment. Other Interventions will be excluded. Interventions in Western medicine group will include antidiarrheal agents, psychotropic agents, and smooth muscle relaxants.
3. Data source and data collection procedures
1) Database for searching
Eleven electronic databases will be searched up to April 2023. Four English databases, including Medline (via PubMed), EMBASE, Cochrane Central Register of Controlled Trials, and Allied and Complementary Medicine Database will be included. Five Korean databases, including the Korean Studies Information Service System, National Digital Science Library, Korean Medical Database, KoreaMed, and Oriental Medicine Advanced Searching Integrated System, will be searched. One Chinese database (China National Knowledge Infrastructure), and Japanese databases (Citation Information by NII) will be included. The researchers will use the term related to the disease and intervention. The search strategy for MEDLINE (via PubMed) is presented in Table 1. There will be no language restriction.

Search Terms for Medline via PubMed
2) Data selection and exclusion
Two researchers (K-WL and S-JK) will independently screen for eligibility and review titles, abstracts, and full texts. The final studies will go through an agreement procedure between the two researchers, and if they disagreed, a third reviewer (JWP) will intervene and resolve it. The screening of the study will be done using the Endnote X7 (Clarivate Analytics, London, UK). This procedure will be illustrated in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram (Fig. 1).
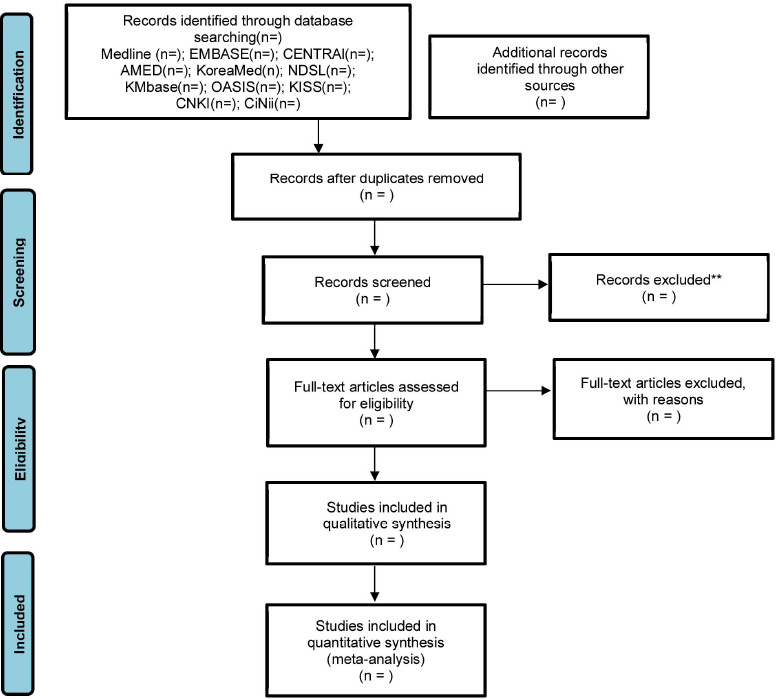
Preferred reporting items for systematic reviews and meta-analyses flow diagram of literature screening and selection process.
AMED = Allied and Complementary Medicine Database, CENTRAL = Cochrane Central Register of Controlled Trials, CiNii = Citation Information by Nii, CNKI = China National Knowledge Infrastructure, KISS = Korean studies Information Service System, KMbase = Korean Medical Database, NDSL = National Digital Science Library, OASIS = Oriental Medicine Advanced Searching Integrated System.
3) Data extraction
Data extraction will be performed using the format “Consolidated Standards of Reporting Trials Extension for Chinese Herbal Medicine Formulas 2017.” It contains various information about the title, abstract, keywords, introduction, trial method, result data, discussion, and others15. Missing or insufficient data will be requested from the corresponding authors of the studies.
4. Quality assessment
The studies will be evaluated using the Cochrane Collaboration’s risk-of-bias tool, which is used to evaluate the bias of the domains, such as random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, completeness of outcome data, selective reporting, and other biases16.
We will use the Grading of Recommendations Assessment, Development, and Evaluation approach to score the quality of evidence. Two researchers will assess the risk of bias, inconsistency and imprecision of the results, indirectness of evidence, publication bias, large effects, and dose-dependent gradients17.
5. Data analysis and synthesis
1) Analysis and synthesis strategy
The Review Manager version 5.3 software (Cochrane Collaboration, Oxford, UK) will be used to process the data. The dichotomous outcome is shown as a risk ratio with a 95% confidence interval (CI), whereas the continuous outcome is shown as a mean difference or standardized mean difference with a 95% CI. Statistical heterogeneity among pooled studies will be calculated using the I² statistic, and if the studies show significant heterogeneity (I²≥50%), the random-effects model will be used. A sensitivity analysis will be performed, if needed.
2) Analysis of subgroups or subsets
A subgroup analysis will be conducted regarding the type or dose of treatment, treatment duration, or the subtype of IBS (diarrhea- or constipation- predominant IBS).
III. Discussion
The global prevalence of IBS in Asia was 9.6%18. Western medicine has not provided the satisfactory results for IBS, leading to recurrent symptom-relapse and economic burden on society19.
Although YGT has long been used to treat gastrointestinal symptoms8, its efficacy and safety in IBS have not yet been fully investigated. A recent studies revealed that YGT showed significant better effect on IBS symptoms compared to that of Western medicine or probiotics20,21. According to Traditional Asian Medicine theory, IBS belongs to the spleen-deficiency and qi-stagnation syndromes; therefore, YGT which boosts the qi of the spleen can be a suitable treatment for IBS22.
In this review, we aimed to determine the statistical efficacy of YGT in the treatment of IBS. This study will provide evidence on the efficacy and safety of YGT as an alternative treatment for IBS, and the results will be beneficial for both the patients with IBS and healthcare providers.
One expected limitation will be the poor quality of the studies including methodology. And another will be insufficient data. Despite above limitations, this review will expand our understanding using YGT for IBS. We hope this study will provide helpful guideline of Korean medicine for IBS.
Registration
PROSPERO ID: CRD42023400078 (https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=400078)
Acknowledgments
This work was supported by a National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2022R1C1C1004937) to S.J.K., and by the Bio & Medical Technology Development Program of the National Research Foundation (NRF) funded by the Korean government (MSIT) (No. 2022M3A9E4082682) to J.W.P..
Author contributions
Conceptualization: Seok-Jae Ko, Jae-Woo Park.
Funding acquisition: Jae-Woo Park.
Methodology: Kangwook Lee, Seok-Jae Ko, Minjeong Kim, Chaehyun Park, Min-Seok Cho.
Supervision: Jae-Woo Park.
Writing - original draft: Kangwook Lee.
Writing - review & editing: Seok-Jae Ko, Jae-Woo Park.
