항암화학요법 유발 말초신경병증에 대한 침치료의 효과: 체계적 문헌고찰 및 메타 분석
The Therapeutic Efficacy of Acupuncture for Chemotherapy-Induced Peripheral Neuropathy: A Systematic Review and Meta-Analysis
Article information
Abstract
Objective:
This study aimed to report the therapeutic effect of acupuncture on chemotherapy-induced peripheral neuropathy (CIPN).
Methods:
The articles were sourced from databases including PubMed, EMBASE, Cochrane Library, CNKI, CiNii, WHO ICTRP, JSOM, KMBASE, KISS, NDSL, and OASIS as of July 2019. The main search keywords were peripheral neuropathy and acupuncture, and only randomized controlled trials using acupuncture for therapeutic purposes were included. Cochrane’s risk of bias was used to assess the risk of bias, and the Review Manager 5.3 program was used for meta-analysis.
Results:
Six studies with a total 394 participants were included. When combined treatment of acupuncture and usual care was compared with usual care alone, quality of life improved more significantly in the combination treatment group (SMD=-2.71, 95% CI: -5.01 to -0.41, P=0.02, I2=97%). The CIPN pain score was lower among the combination treatment group, but not to a significant degree (SMD=-2.55, 95% CI: -5.14 to 0.04, P<0.05, I2=98%). There were no severe side effects in any studies.
Conclusion:
Acupuncture combined with usual care may be considered to safely relieve CIPN pain and improve quality of life for cancer patients. However, as there are few randomized controlled trials studying the effect of acupuncture on CIPN, further well-designed research is needed.
I. 서 론
국내에서 가장 많은 사망원인을 차지하고 있는 암은 전 세계적으로도 인구의 증가와 고령화 등으로 인해 발생 및 사망자 수가 매년 증가하고 있다1,2. 항암화학요법(chemotherapy)은 종양의 억제를 목적으로 사용하는 표준치료 중 하나로 암 환자의 60-75%가 시행한다. 그러나 반복적으로 장기간 항암화학요법을 받는 암 환자는 강한 독성으로 인한 광범위한 세포 파괴로 전신적인 부작용을 경험할 수 있다3. 그 중 탁산계(taxane), 플래티늄계(platinum), 빈카알칼로이드계(vinca alkaloids), 탈리도마이드계(thalidomide), 볼테조밉(bortezomib) 등 계열의 항암제를 사용하는 환자의 38-70%에서 말초의 운동, 감각 및 자율신경계가 손상되어 항암화학요법 유발 말초신경병증(chemotherapy induced peripheral neuropathy, CIPN)이 발생하여 통증, 저림, 냉감, 작열감, 감각 소실, 이상감각 등의 감각 장애, 근력 저하, 근육 경련과 같은 운동 장애의 증상이 나타난다4-6.
CIPN은 항암화학요법으로 유발되는 부작용에서 골수기능부전에 이어 두 번째로 빈도가 높은 신경독성 부작용 중 하나이며 주로 유방암, 혈액암, 대장암, 위암 환자에서 흔히 발생한다7. 말초신경병증은 신경독성 항암제가 축적되면서 신경 축삭을 감싸는 수초의 손상으로 말초신경 조직의 파괴나 변성이 일어나 발생하며 치료 종료 후에도 수개월에서 수년간 지속될 수 있고 심한 경우 불가역적인 후유증을 남긴다8. 후유증이 지속되면 삶의 질 저하와 신체기능 저하를 유발할 뿐만 아니라 암에 대한 표준치료의 효과를 감소시키거나 치료를 지연시킬 수 있기 때문에 증상 완화를 위한 다양한 치료법이 제시되고 있다. 임상적으로 CIPN의 치료를 위해 gabapentin과 pregabalin과 같은 항경련제, 마약성 진통제, tricyclic계 항우울제 등의 약물적 치료와 신경자극술, 재활치료, 도수치료와 같은 비약물적 치료가 통용되고 있으나 아직 그 효과들에 대한 근거가 부족하여 유효성이 증명되고 있지 않으며, 최근 들어서 serotonin and noradrenaline reuptake inhibitor(SNRI)계 항우울제인 duloxetine에 대한 권고만 제시되고 있다9-11.
최근 세계적으로 암에 대한 한의학적 치료의 관심이 높아지면서 침치료가 암성 통증, 암성 피로, 오심구토 및 상열감 등의 항암화학요법 유발 부작용, 방사선요법 유발 구강건조증과 같은 암 관련 증상과 암 환자의 치료율 및 삶의 질에 긍정적인 효과가 있으며 이로 인해 생존율을 증가시킨다는 여러 연구가 발표되고 있다12-14. 또한 침치료는 미국, 중국, 유럽 등의 연구에서는 당뇨, 벨마비, 터널증후군 등의 기저질환에 의해 유발되는 말초신경병증에서도 유의한 효과가 보고되었다. 뿐만 아니라 유방암, 림프암, 기관지암, 대장암 등 다양함 암 종 환자에서의 CIPN에도 침치료의 유효성에 대한 연구가 진행되고 있으며 일부 유효한 효과가 보고되어 임상적으로 다수 활용되고 있다15-17.
그러나 현재 CIPN에 대하여 침의 치료적 유효성과 예방적 유효성이 혼재되고 있으며 선행 연구에서 아직 일관된 결과가 없고 대규모 연구의 부재로 적극적으로 권고함에 있어서는 근거가 부족한 현황이다18. 이에 본 연구에서는 침의 CIPN에 대한 치료적 효과를 평가하고자 영어, 일본어, 중국어의 언어로 작성된 다국적 연구에 대하여 문헌 고찰 및 메타분석을 시행하였다.
II. 연구 방법
1. 검색 전략
2019년 7월까지 발표된 논문을 대상으로 영어 문헌은 PubMed, EMBASE, Cochrane Library, WHO ICTRP, JSOM, 중국어 문헌은 CNKI, 일본어 문헌은 CiNii, 국내 문헌은 KMBASE, KISS, NDSL, OASIS를 이용하여 2019년 8월부터 2020년 1월까지 검색하였다.
항암화학요법 유발 말초신경병증에 대한 침치료 연구를 검색하기 위해 “(Neoplasms OR cancer OR tumor OR malignant OR drug therapy or antineoplastic agents) AND (peripheral nervous system diseases OR peripheral neuropathy OR neuralgia) AND (Acupuncture OR acupoint OR electroacupuncture OR bee venom OR pharmacopuncture OR herbal acupuncture)”를 검색어로 검색하였다. 또한 모든 문헌 검색에 대하여 각 데이터베이스에서 무작위 대조군 연구를 시사하는 검색어를 포함하여 연구 유형을 제한하였다.
2. 선정 기준 및 제외 기준
검색된 논문의 제목과 초록을 통해 1차로 확인하고, 이후 논문의 원문을 검토하여 다음의 기준을 충족시킬 때 포함하였다. (1) 항암화학요법 유발 말초신경병증을 호소하는 환자, (2) 증상의 중재술로 일반침, 전침, 봉침, 약침 등의 침치료를 사용한 환자, (3) 무작위 대조군 임상 연구, (4) 침치료를 치료적 목적으로 사용한 연구, (5) 한국어, 중국어, 영어, 일본어로 작성된 논문의 전문을 확인할 수 있는 문헌이 포함되었다. 반면 다음의 기준에 해당될 경우 배제하였다. (1) 회색 문헌, (2) 침치료를 예방적 목적으로 사용한 연구. 회색 문헌은 학위 논문, 초록만 발표된 문헌, 프로토콜 논문, 레터 및 기타 보고서로 정의하였다. 선별 과정에서는 두 명의 저자(KEH, YSW)가 참여하였으며, 두 명의 결과물을 비교 및 합의하는 중에 이견이 있을 경우 제 3의 연구자(LJY)와 토의하여 최종 문헌을 선택하였다.
3. 비뚤림 위험 평가
비뚤림 위험 평가는 Cochrane group이 제작한 Risk of Bias(RoB)19 도구를 사용하여 수행되었다. 무작위 배정순서 생성, 배정순서 은폐, 연구참여자 및 연구자 눈가림, 결과 평가자 눈가림, 불충분한 결과 자료, 선택적 결과 보고, 그 외 비뚤림의 7가지 항목에 대해 “높음(high risk of bias)”, “주어진 자료가 불충분함(unclear risk of bias)”, “낮음(low risk of bias)”로 평가하여 표기하였다. 평가의 세부 기준은 NECA 체계적 문헌 고찰 매뉴얼20을 참고하여 시행하였으며 검토자 간에 의견이 일치하지 않을 경우 제 3자로부터 의견을 구해 재논의 하였다.
4. 메타 분석
메타 분석은 분석 가능한 동일한 결과 변수를 보고한 연구가 3편 이상 있을 때 수행하였다. 중재의 효과 크기는 Cochrane Library의 Review Manager Version 5.3 프로그램으로 산출하였으며, 이분형 자료는 상대위험도(risk ratio, RR)와 95% 신뢰구간을 이용하고 연속형 자료는 표준화된 평균차(standardized mean difference, SMD)와 95% 신뢰구간으로 표시하였다. 개별 연구 간에 이질성을 고려하여 변량 효과 모형(random effects model)을 이용하였고 대상 연구의 동질성 여부는 I2 검정을 통해 확인하였다. I2값은 이질성이 없을 때 0%이며, 중등도의 이질성이 50-75%, 75% 이상은 고도의 이질성을 의미한다21.
III. 결 과
1. 문헌 선정
국내외 11개의 데이터베이스를 통해서 2019년 7월까지 발표된 문헌 총 599편이 확인되었다. 그 중 중복 문헌을 제거하여 507편을 선별하였고 초록과 제목을 검토하여 주제와 선정 기준에 연관이 없는 문헌 375편을 배제하여 132편을 1차 선별하였다. 선별된 132편을 대상으로 본문을 검토하여 항암화학요법 유발 말초신경병증과 관련 없는 논문(n=3), 침치료를 중재로 사용하지 않은 논문(n=7), 무작위 대조군 연구가 아닌 논문(n=90), 침치료를 증상의 예방적 목적으로 사용한 논문(n=3), 원문 확보가 불가능한 논문(n=18), 회색 문헌(n=3), 중복되어 출판된 논문(n=2)을 제외하여, 총 6편의 논문22-27을 선택하였다(Fig. 1).
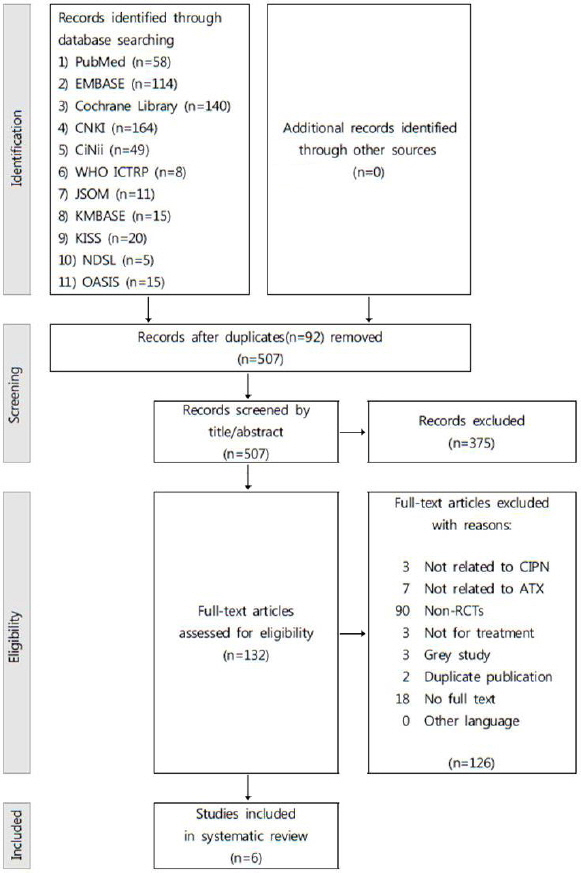
Flow diagram of study screening.
2. 연구 특성
394명의 참가자가 포함된 6편의 선정 논문의 특성은 Table 1에 요약하였다. 암 종은 유방암23-27과 혈액암22-25 환자가 가장 많았으며 이외에는 위장관계암, 비뇨생식계암, 난소암, 두경부암이 있었다. 말초신경병증을 유발한 항암화학요법 약물의 종류에 대해서는 taxane계24-26와 oxaliplatin 항암제24,26가 주를 이루었으나 6편 중에 3편22,23,27이 해당 사항에 대하여 언급한 바가 없었다. 6편 중 3편22,23,25은 침치료와 통상치료의 병행과 통상치료 단독치료의 효과를 비교한 논문이었으며, 2편26,27은 침치료 단독치료와 통상치료 단독치료의 효과를 비교한 논문이었고, 다른 1편24은 4-arm RCT로 전침을 수중전자목욕(hydroelectric baths), 고용량 비타민 B 복합체 캡슐, 젖당 캡슐과 비교한 논문이었다. 선정된 논문에서 보고된 치료 기간은 2주에서 12주였으며 치료 효과에 대한 추적관찰 기간은 2주에서 20주였다. CIPN의 증상은 관련 증상의 강도, 삶의 질, 신경전도검사, 치료 반응률의 범주로 평가되었다.

The Characteristics of the Included Randomized Controlled Trials
3. 비뚤림 위험 평가
선정된 6편의 비뚤림 위험 평가 결과는 Table 2에 제시하였다. 선택 비뚤림에서는 YANG27의 연구 경우 무작위 배정 과정에서 병원 방문 순서에 따라 배정하였다는 보고를 고려하여 무작위 배정순서 생성과 배정순서 은폐에 관한 비뚤림을 ‘높음’으로 평가하였다. 다른 5편22-26의 연구 모두 무작위 배정순서 생성에 관한 비뚤림은 ‘낮음’에 해당하였으나 그 중 2편22,26은 배정순서 은폐에 관한 내용을 구체적으로 언급하지 않아 ‘불확실’로 평가하였다. 실행 비뚤림에서는 6편의 논문 모두 침치료와 통상치료를 비교한 문헌으로 연구참여자 혹은 연구자에 대한 눈가림이 불가능하여 ‘높음’에 해당되었다. 검출 비뚤림에서는 1편23의 논문에서만 결과 평가자의 눈가림을 보고하여 ‘낮음’에 해당되었으며 다른 5편22,24-27은 모두 언급하지 않아 ‘불확실’로 평가하였다. 탈락 비뚤림에 대해서는 YANG27의 연구 경우 환자 탈락에 대한 언급이 없어 ‘불확실’로 평가하였으며 다른 5편22-26의 경우 양 군 환자의 탈락이 적고 탈락율이 비슷하여 ‘낮음’에 해당하였다. 결과보고 비뚤림에서는 XU26의 연구만 ‘불확실’에 해당되며 다른 5편22-25,27은 모두 ‘낮음’으로 평가하였고 모든 문헌에서 기타 비뚤림은 존재하지 않았다(Fig. 2).

Risk of Bias in the Included Randomized Controlled Trials
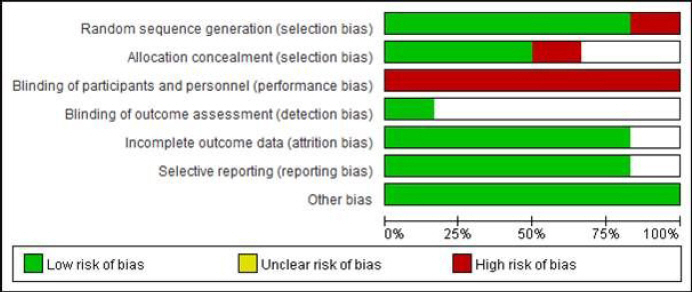
Risk of bias graph of the included randomized controlled trials.
4. 치료 효과
1) 침치료 및 통상치료의 병행 전후 통증 강도 비교
3건의 문헌22,23,25으로 메타분석을 시행하여 침치료 및 통상치료 병행 전후의 visual analogue scale (VAS) 및 brief pain inventory(BPI)로 평가한 통증 강도 점수를 비교하여 분석한 결과 통상치료 단독에 비하여 증상이 호전되었으나 유의하지는 않았다(SMD=-2.55, 95% CI: -5.14 to 0.04, P<0.05, I2=98%)(Fig. 3).
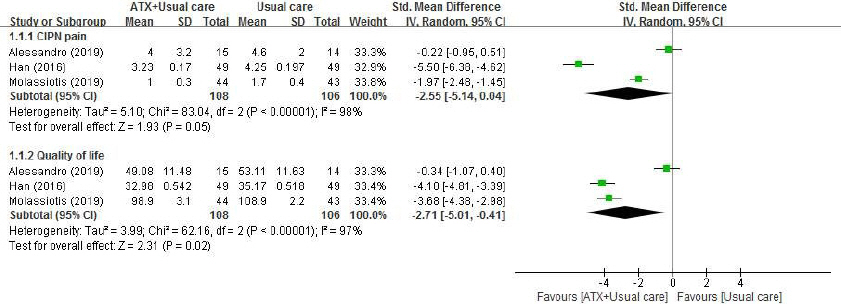
Meta-analysis of acupuncture treatment in symptom intensity and quality of life for chemotherapy-induced peripheral neuropathy patients.
ATX : acupuncture, CIPN : chemotherapy induced peripheral neuropathy
2) 침치료 및 통상치료의 병행 전후 삶의 질 비교
3건의 문헌22,23,25으로 메타분석을 시행하여 침치료 및 통상치료 병행 전후의 FACT/GOG-Ntx (Functional Assessment of Cancer Therapy/Gynecologic Oncology Group-Neurotoxicity), EORTC QLQ-C30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Core 30)으로 평가한 삶의 질 점수를 비교하여 분석한 결과 통상치료 단독에 비하여 삶의 질이 유의하게 호전되었다(SMD=-2.71, 95% CI: -5.01 to -0.41, P=0.02, I2=97%)(Fig. 3).
IV. 고 찰
항암화학요법을 받은 암 환자의 항암화학요법 유발 말초신경병증에 있어 침치료의 효과를 종합적으로 검토하고자 본 연구를 계획하였다. 침치료에는 일반침, 전기침, 이침, 지압(Acupressure), 봉침, 약침 치료를 포함하였으며 침치료의 예방적 유효성과 치료적 유효성의 혼재를 막고자 치료적 효과에 대한 무작위 대조군 문헌으로만 제한하였다. 최종적으로 선정된 6건의 논문을 종합한 결과, 침치료와 통상치료의 병행은 통상치료 단독 치료와 비교했을 때 FACT/GOG-Ntx 설문지와 EORTC QLQ-C30 설문지로 평가한 삶의 질을 유의하게 호전시켰다. VAS와 BPI 설문지로 측정한 CIPN 통증 강도에서도 통증 점수가 보다 낮은 경향이 있었으나 통계적으로는 유의하지 않았다. 6건의 문헌 중 침치료가 CIPN과 관련된 증상 및 삶의 질에 효과가 없었던 유일한 연구는 Rostock et al24의 연구로, 전기침, 수중전자목욕(hydroelectric baths), 고용량 비타민 B1/6 복합체 캡슐, 젖당 캡슐을 비교하여 침치료를 3주간 약 8회 시행한 결과 각각의 중재군 간에 유의한 차이가 없는 것으로 나타났다. 이러한 결과에 대하여 해당 연구에서는 포함된 대상자들의 CIPN이 매우 중증 이였으며 대조군으로써 비교할 수 있는 정상군의 부재가 관련된 것이라 보고하였다. 부작용에 대해서는 6건의 논문 중 4건에서 부작용 여부를 보고하였으며 그 중 1건에서만 경도의 부작용이 나타났다. 경도의 부작용에는 무기력, 현기증 등이 있었으나 침치료를 시행한 환자가 통상치료를 시행한 환자에 비해 부작용이 유의하게 적었다. 따라서 침치료와 통상치료의 병행은 항암화학요법 유발 말초신경병증을 호소하는 암 환자에게 고려할 수 있는 안전한 방법이며 위해보다는 잠재적인 이득의 효과가 클 것으로 판단된다.
CIPN은 항암화학요법을 시행하는 암 환자의 38-70%에서 나타나는 신경손상 병증으로 통증, 저림, 마비감 등의 증상이 양측성으로 손과 발의 원위부에서부터 시작되어 진행된다. 또한 “stocking-glove” 양상의 임상 형태를 보이는데 이는 길이가 긴 신경이 먼저 손상되는 특성에 따라 발목까지 증상이 진행되면 손 끝 마디로, 무릎까지 진행되면 손목으로 증상이 올라오는 양상을 의미한다28. 항암제가 신경손상을 일으키는 기전은 암세포에 대해 항암 효과를 일으키는 기전과 유사하여 vinca alkaloids, taxane, platinum, thalidomide, bortezomib 계열 항암제가 신경섬유 DNA 내에 화합물을 생성하여 삼차구조를 변형시킴으로써 탈수초화, 축삭 괴사 등의 신경섬유 변형, 신경세포 파괴 및 재생 억제를 야기하여 CIPN이 유발된다. CIPN은 항암제의 종류, 용량, 투여 기간, 연령, 당뇨병 등의 신경계 병증을 악화시킬 수 있는 기저질환 유무, 다른 약물 사용력 등에 따라 증상이 수년 간 지속되거나 비가역적인 후유증을 유발할 수 있어 삶의 질에 악영향을 미칠 뿐만 아니라 표준치료의 지연도 야기할 수 있어 적극적인 관리가 요구되는 부작용 중 하나이다. 그러나 현재까지 gabapentin 성분의 항경련제, 삼환계 항우울제, 마약성진통제, 비타민 B 등 CIPN이 아닌 다른 신경병증에서 유효성이 증명된 약물적 치료제를 기반으로 CIPN에 대한 효과를 다양하게 연구하였으나 일관된 결과가 부족한 현황이다21. 그 중 Ellen et al11의 연구에서 당뇨병성 신경병증과 섬유근육통에 통용되는 SNRI계 항우울제인 duloxetine이 paclitaxel과 oxaliplatin으로 CIPN이 유발된 암 환자에서 CIPN 통증에 대하여 통증 강도 감소치의 평균이 플라세보 대비 통계적으로 유의하게 큰 것(1.06, 95% CI: 0.72 to 1.40 vs 0.34, 95% CI: 0.01 to 0.66; p=0.003)이 보고되어 2014년 미국임상종양학회에서 중등도로 사용하도록 제안하였다. 그러나 고령의 환자에서는 장복의 항우울제가 부작용을 일으킬 수 있으며29, 여전히 국내외적으로 CIPN에 대하여 정립된 권고 치료가 없는 상태에서 대체보완적인 중재에 대한 수요가 증가하고 있다21.
침치료는 말초 자극을 통해 혈류량을 증가시킴으로써 신경 내 혈관의 혈류 순환을 촉진시키며 이는 신경세포의 수초와 축삭의 재생을 도모해 손상된 말초신경의 회복을 돕는 것으로 알려져 있다30,31. 또한 침치료로 유발된 말초신경의 자극은 중추신경계의 통증억제경로를 활성화시켜 진통 효과도 나타내기 때문에32 American Cancer Society(ACS)와 American Society of Clinical Oncology(ASCO)의 가이드라인에 따르면 유방암 환자의 통증에 침치료가 높은 근거 수준으로 권고되고 있다33. 말초신경병증에 대해서는 당뇨병34, 후천성면역결핍증35으로 유발된 말초신경병증에 침치료의 유효한 효과가 보고되면서 CIPN에 대한 연구도 진행되기 시작하였는데 현재 폐암환자의 통합종양학 임상진료지침에서 약물적 통상치료에도 조절되지 않으며 임상적으로 CIPN 관련 증상이 환자의 삶의 질에 주요한 영향을 미치는 경우 증상 완화를 위해 침치료를 시도해볼 것으로 제안되어 있다36. 또한 National Comprehensive Cancer Network(NCCN)의 지침에서는 암 환자의 제반 신경성 통증에 침치료를 시행하여 긍정적인 효과를 기대할 수 있지만, 항암화학요법 유발성 증상의 경우 약물적 치료에도 조절되지 않는 경우에 시도할 수 있는 선택지라고 보고하였다37. 앞선 진료지침들의 첨언에 따르면 침치료의 CIPN에 대한 권고가 등급이 낮은 원인으로 양질의 선행연구 부족과 일관된 연구결과의 부재를 공통적으로 꼽았는데 이에 대하여 2019년 Chien et al38의 CIPN에 대한 침치료의 다국적 문헌을 포함한 최초의 메타분석 연구가 보고되었다. 6건의 문헌을 포함하였는데 그 중 3건이 본고와 동일하였고, 분석 결과 침치료는 CIPN 통증 감소(-1.21, 95% CI -1.61 to 0.82; p<0.00001), FACT/GOG-Ntx로 평가한 신경계 증상 호전(-2.02, 95% CI -2.21 to -1.84; p<0.00001)의 효과가 있었기에 비약물적 치료제로써의 가능성을 제시하였다. 그러나 해당 연구의 메타분석 과정에서 통상치료 병행 여부를 일치시키지 않은 것, 대조군의 중재에서 통상치료와 플라세보 침을 혼재한 것, 예방적 목적과 치료적 목적의 연구를 구분하지 않은 등의 제한점이 있었기에 본고에서 이를 반영하여 연구를 설계하였고 그 결과 침치료와 통상치료 병행이 CIPN을 호소하는 암 환자의 삶의 질에 유의한 효과가 있음을 보고하였다.
본고에서는 다음의 제한점이 있다. 첫째로 포함된 6건 문헌의 총 대상자 수가 394명으로 대규모 문헌고찰을 시행하지 못한 점으로, 이는 현재 CIPN에 대한 침치료의 효과를 분석한 선행 무작위 대조군 연구의 부족이 영향을 미친 것으로 사료된다. 둘째로 항암화학요법 유발 말초신경병증이 환자가 호소하는 임상적 증상으로 진단하고 평가하는 병증임을 고려했을 때 증상 혹은 삶의 질의 평가에 있어서 환자의 주관적인 비뚤림이 존재할 수 있는 점이다. 그러나 본고에서 다국적 무작위 대조군 문헌을 포함하여 체계적 문헌고찰 및 메타분석을 시행하여 침치료의 유의한 치료적 유효성을 증명한 것은 이미 국내에서 항암화학요법 유발 말초신경병증에 대하여 침치료가 임상적으로 다빈도 사용되고 있는 현황에 대한 근거로써 의의를 가진다. 향후 신경전도검사와 같은 정량적 평가 도구를 사용하여 대규모 임상 연구를 시행함으로써 보다 높은 한의학적 치료 가치를 확인할 수 있을 것으로 사료된다.
감사의 글
본 연구는 한국보건산업진흥원을 통해 보건복지부 「한의약선도기술개발사업」의 재정 지원을 받아 수행된 연구임(과제고유번호: HB16C0067).