두통으로 한방병원에 내원하여 컴퓨터단층촬영후 지주막하출혈로 진단된 증례 보고
Case Series of Headache Patients Diagnosed with Subarachnoid Hemorrhage by Computed Tomography in a Korean Medicine Hospital
Article information
Abstract
The purpose of this study was to investigate the cases diagnosed as subarachnoid hemorrhage by noncontrast computed tomography (NCCT) after the appearance of symptoms related to headache and paralysis in patients who visited a Korean medicine hospital. A search of electronic medical records of patients diagnosed with subarachnoid hemorrhage on NCCT in W Korean medicine hospital from January 2010 to December 2017 identified five patients. The patients (four women and one man) ranged in age from 64 to 79 years old. Three were inpatients and two were outpatients. Two patients had hypertension, two patients had diabetes, two patients had heart disease, and two patients had a history of cerebral infarction. Development of a cooperative system is needed for accurate diagnosis and appropriate treatment of this disease in the Korean medicine clinic and for establishment of an NCCT scan application method.
I. 서 론
두통을 호소하는 성인에서 가장 위험한 응급 상황으로 즉시 적절한 의뢰나 검사 등의 대책을 세워야 하는 것으로는 벼락두통의 발생, 발열과 수막자극증상, 국소 증상이나 의식의 상실을 동반한 시신경유두부종, 급성 녹내장으로 인한 두통이 있다1. 벼락 두통은 발병시에 최대 강도를 가지는 급성의 심한 두통이다. 벼락두통의 여러 원인 중에서 지주막하출혈(subarachnoid hemorrhage, SAH)은 가장 흔한 원인이며, 정확한 진단을 위해서는 영상의학 검사를 시행한다2. SAH의 확진을 위해서는 컴퓨터단층촬영(computed tomography, CT)과 요추천자가 사용되는데 발병 수시간 이내에 적절히 시행된다면 CT는 거의 100%의 민감도와 특이도를 보이므로 요추천자를 시행하지 않아도 충분하다3.
지주막하 출혈의 연간 발생률은 100,000명당 5-20명이며, 이 중 25-50%가 발병 30일 내에 사망하고, 특히 비외상성 지주막하 출혈은 병원 전 심정지의 신경학적 원인 중 제일 많은 원인 질환이며, 출혈 직후 심정지가 합병되지 않은 환자군의 30%도 결국 발병 24시간 내에 사망한다. 따라서 SAH는 증상이 의심되었을 때, 적절한 검사와 진단을 받는 것이 무엇보다 중요하다고 볼 수 있다4,5.
우리나라는 1951년 의료법의 제정이후 한방과 양방의 의료이원화체계를 유지해 오고 있으며, 1990년대 이후 한방과 양방 교류의 필요성이 제기되면서 상호 보완적 진료의 방안이 모색되고 있고, 협진의 노력은 증대되고 있다6. 또한 협진 분야에 있어서는 뇌졸중, 근골격계 질환, 면역계 질환 등이 높은 순위를 차지하고 있다. 그러나 여전히 협진에 대한 부정적인 인식은 존재하며, 효과적인 협진의 방식들이 제안되고 있지 못한 실정이다7.
SAH의 한의 임상 관련 연구는 지주막하출혈의 직접적인 진단 및 치료와 관련된 것은 없으며, 지주막하출혈로 인한 어지러움과 이명이 한의학적 치료로 호전된 증례만이 확인되었다8,9.
본 연구는 두통 및 중풍과 관련된 증상이 발생한 후 한방병원에 내원한 환자를 영상의학과에 의뢰하여 CT를 시행하여 지주막하출혈로 진단된 증례를 정리한 연구이다. SAH로 진단된 환자 5명의 발생시 증상, 위험 인자, CT 소견 등을 정리하였다. 본 논문이 한방의료기관에서 두통 환자 진단, 치료 방향 결정, 협진의 필요성 제시 및 구체적 마련 등에 의미가 있는 증례로 활용될 수 있으리라 생각되어 보고하는 바이다.
II. 증 례
1. 전체적 특징
2010년 1월부터 2017년 12월까지 W한방병원의 전자의무기록을 검색하여 비조영증강 컴퓨터단층촬영(noncontrast computed tomography, NCCT)상 지주막하출혈(subarachnoid hemorrhage, SAH)로 진단된 환자를 검색하였다. 검색결과 5명의 환자가 확인되어, 의무기록에 근거하여 고혈압, 당뇨병, 심장병, 뇌졸중 등의 질환 유무를 비롯한 환자 정보와 발병 경과, 치료 내용을 확인하여 정리하였다. 확인된 환자의 나이는 최저 64세, 최고 79세이었다. 여성은 4명이었으며, 남성은 1명이었다. 3명은 입원 환자이었으며, 2명은 외래 환자이었다. 2명에서 고혈압이 있었으며, 2명에서 당뇨병이 있었으며, 2명에서 심장병이 있었으며, 2명에서 뇌경색의 과거력이 있었다. 한의학적 변증은 氣鬱, 陰虛, 氣虛 등 다양하였으며, 발병 이전에 滋陰降火湯, 獨活寄生湯, 淸上蠲痛湯 등이 투여되었다(Table 1).

Characteristics of the Patients Diagnosed as Subarachnoid Hemorrhage by Noncontrast Computed Tomography
2. 증례 1(77세 여성, 입원 환자)
1) 환자 정보
내원 당시 만 77세의 여성으로 기관지 천식, 심장 수술, 고혈압, 뇌경색의 과거력이 있었다. 2010년 7월 ⃝⃝일에 두통과 어지러움이 발생하였다. 두통 발생 10일후 자기공명영상촬영(magnetic resonance imaging, MRI)에 의해 뇌경색으로 진단되었다. 두통 발생 12일후 한방병원에 입원하였으며, 내원 당시 주소증은 눈이 쏟아질 듯한 통증, 두피 마비감, 어지러움이었으며, 입원 당시 혈압은 110/70 mmHg이었다. 입원 중 활력징후는 혈압은 90-130/60-80 mmHg, 체온은 36.2-36.5 °C, 맥박수는 60-80 times/min, 호흡수는 20-22 times/min으로 비교적 안정적이었다. 두통 발생 19일후인 입원 7일째에 어지러움이 호전되어 단독 보행이 가능하였으며, 두통 발생 26일후인 입원 14일째에 집으로 외출을 하였다.
2) 발병 경과
두통 발생 27일후인 입원 15일째 오전 10:00경에 보호자가 전화를 걸어 환자가 아침에 머리를 감던 중 갑자기 심한 두통과 구토가 갑자기 발생하여 구급차로 한방병원으로 오는 중이라고 하였다. 환자는 오전 10:30에 도착하여 확인하니 정신상태는 명료하였다. 두통, 어지러움, 구토, 오한을 호소하였으며, 혈압은 160/100 mmHg, 맥박수는 100 times/min이었다. 오전 11:20에 NCCT상 SAH로 진단되었다. 오전 11:25에 혈압 200/100 mmHg, 오전 11:30에 혈압 170/100 mmHg로 측정되었다. 환자는 상급 의료기관으로 전원하였다(Fig. 1).

Noncontrast computed tomography image of the 77-year-old woman.
She had hypertension, heart disease, and cerebral vascular disease history, who was diagnosed with acute subarachnoid hemorrhage. Abnormal blood collection in left prepontine cistern (arrow) and left basal cistern (arrowhead) are observed.
3) 치료 내용
환자는 입원 중에는 침, 부항을 시행하였으며, 한약 처방은 자음식풍탕, 청상견통탕, 제병통치환, 천금광제환, 우황청심원 등을 사용하였다. 양약은 J병원의 처방전에 의해 아스트릭스, 아프로벨, 바이토린, 나페론씨알, 베타원, 파라마셋, 알비스, 프레탈, 케타스, 알프람, 씨베리움, 글리아티린, 맥스마빌, 아미노피, 비오콘틴을 복용중이었다.
3. 증례 2(78세 여성, 입원 환자)
1) 환자 정보
내원 당시 만 78세의 여성으로 뇌경색, 당뇨병의 과거력이 있었다. 2010년 3월 ⃝⃝일에 좌측 반신마비가 발생하여 G대학교병원에서 MRI상 우측 전대뇌동맥의 뇌경색과 우측 A3 영역의 협착으로 진단받은 후 13일간 입원치료를 하였다. 반신마비 발생 13일후 한방병원에 좌측 반신마비, 말어둔, 두통, 현훈, 정신상태 명료 및 기면을 주소로 내원하여 2010년 3월 ⃝⃝일부터 7월 ⃝⃝일까지 총 125일간 입원하였다. 입원 중 혈압은 110-130/60-80 mmHg로 비교적 안정적이었다. 입원 중 간기능 수치 상승, 요로계 감염, 폐렴 등의 합병증이 발생하여 치료하여 완치되었다.
2) 발병 경과
입원 125일째인 7월 ⃝⃝일 오후 12:25에 갑자기 오심, 구토가 발생하였으며, 혈압이 170/110 mmHg로 측정되었다. 오후 12:35에 혈압이 220/140 mmHg로 측정되었으며, 두통, 하품, 오심, 구토 증상이 지속되어 오후 12:57에 NCCT를 촬영하였다. 촬영 결과 SAH로 진단되어 상급 의료기관으로 전원하였다(Fig. 2).
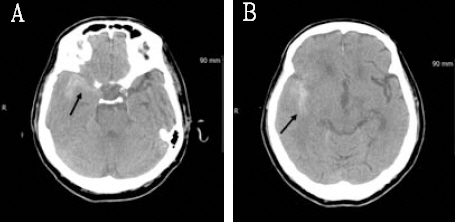
Noncontrast computed tomography image of the 78-year-old woman.
She had heart disease, and cerebral vascular disease history, who was diagnosed with acute subarachnoid hemorrhage. A : Blood collection along the right temporal convexity (arrow) is observed. B : Blood collection along the right sylvian fissure (arrow) is observed.
3) 치료 내용
환자는 입원 중에는 침, 부항을 시행하였으며, 한약 처방은 자음식풍탕, 대시호탕, 향사평위산 등을 투여하였다.
4. 증례 3(74세 여성, 외래 환자)
1) 환자 정보
내원 당시 만 74세의 여성으로 고혈압, 당뇨병 등의 과거력은 없었으며, 골다공증 약을 복용중이었다.
2) 발병 경과
2013년 3월 ⃝⃝일 오전 11:00에 갑자기 두통, 어지러움이 발생하여 한의원을 거쳐서 내원하였다. 당일 오후 12:43에 NCCT상 SAH로 진단받아 상급 의료기관으로 전원하였다. 두통 발생 2일후 서울 G대학교병원에서 코일색전술을 시행하였으며 9일간 입원하였다. 두통 발생 11일째에 서울 G대학교병원에서 퇴원하여 한방병원에 내원하여 입원하였다. 내원 당시 머리 전체가 쿡쿡 쑤시고 애리는 양상의 두통을 호소하였으며, 어지러움, 오심, 구토 등은 없었다. 한방병원에서 10일간 입원하였으며 입원중 혈압은 110-130/70-90 mmHg로 비교적 안정적이었으며, 체온, 맥박수, 호흡수 등도 안정적이었다. 퇴원 후 10일이 경과한 두통 발생 31일째에 두통이 다시 발생하여 SAH 재발을 걱정하며 내원하였으나 NCCT를 시행한 결과 정상 소견을 보여 귀가 조치하였다(Fig. 3).
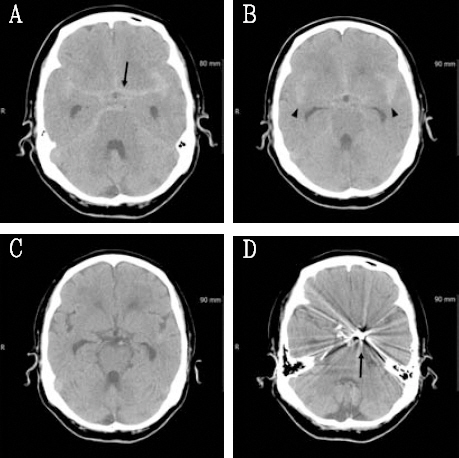
Noncontrast computed tomography image of the 74-year-old woman.
She had no risk factor, who was diagnosed with acute subarachnoid hemorrhage. A, B : Abnormal blood collection in basal cistern (arrow) and both sylvian fissure (arrowhead) are observed. C : Removed state of previous hemorrhage. D : Post-operative state of previous subarachnoid hemorrhage (arrow).
3) 치료 내용
환자는 입원 중에는 침, 부항을 시행하였으며, 한약 처방은 청상견통탕, 성향정기산, 조등산 등을 투여하였다.
5. 증례 4(64세 남성, 외래 환자)
1) 내원 당시 만 64세의 남성으로 당뇨병, 간질환의 과거력이 있었다. 2012년 10월 ⃝⃝일에 좌측 반신마비, 두통, 어지러움, 오심으로 내원하였다. 환자 진술에 의하면 전날 과음하였다고 하였다. 내원 당시 혈압은 150/90 mmHg이었으며, NCCT상 SAH로 진단되어 상급 의료기관으로 전원하였다(Fig. 4).

Noncontrast computed tomography image of the 64-year-old man.
He had diabetes mellitus, who was diagnosed with acute subarachnoid hemorrhage. A, B : Abnormal blood collection along the both cerebello-pontine cisterns (arrows) is observed.
6. 증례 5(79세 여성, 외래 환자)
1) 내원 당시 만 79세의 여성으로 당뇨병, 고혈압의 과거력이 있었다. 2011년 12월 ⃝⃝일 밤에 전신통, 보행장애, 두통, 어지러움, 요각통이 발생하여 다음날 한방병원에 내원하였다. 내원 당시 혈압은 140/80 mmHg이었으며, NCCT상 SAH로 진단되어 상급 의료기관으로 전원하였다(Fig. 5).
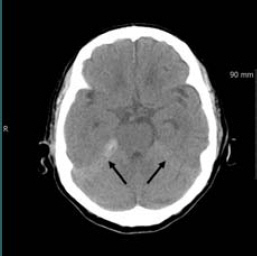
Noncontrast computed tomography image of the 79-year-old woman.
She had hypertension, and diabetes mellitus, who was diagnosed with acute subarachnoid hemorrhage. Abnormal blood collection along the both cerebello- pontine cistern (arrows) is observed.
III. 고찰 및 요약
처음으로 경험하는 심한 두통으로 응급실에 내원하는 환자의 3분의 1 정도가 두개내의 심각한 질환을 가지고 있으며, 이들의 대부분은 지주막하출혈(subarachnoid hemorrhage, SAH)이므로 심각한 두통과 양성 두통을 구별하고 관리하는 일이 중요하다10. 2018년에 한약진흥재단의 보고서에 의하면 외래진료서비스를 이용한 질환 및 증상 25개 중에서 두통은 3.1%로 11번째를 차지하였으며, 입원진료서비스에서는 3.9%로 22개 질환 및 증상 중에서 9번째를 차지하였다11. 따라서 한방의료기관에서도 심각한 두통의 기저 질환을 구별하고 관리하기 위해 진단에 필요한 적절한 검사 기기와 인력을 확보해야 한다. 그러나 두통의 진단시 사용되는 컴퓨터단층촬영(computed tomography, CT), 자기공명영상촬영(magnetic resonance imaging, MRI)은 의사의 지시에 의해서만 시행이 가능한 경우가 많으므로 신속한 의뢰와 적절한 의사소통이 가능한 협진 시스템의 개발이 무엇보다 필요하다고 하겠다.
한의과와 의과 또는 한방과 양방 협진은 진단과 치료의 두 분야에서 이루어지는 경우가 많다. 진단 분야는 혈액검사, 엑스레이, CT 등이 가장 흔한 협진 내용이며, 치료 분야는 수액 처방, 혈압 강하제 투여, 뇌압 강하제 투여, 혈당 강하제 투여가 가장 흔하다. 협진이 이루어지는 질환은 순환기계질환과 근골격계질환이 대부분이다12. 의과와 한의과의 협진 치료는 의과 단독 또는 한의과 단독 치료보다 치료율의 상승, 치료기간의 단축, 치료 만족도의 상승 등에서 유리한 경우가 많다. 협진의 장점은 급성기나 만성기 모두 해당된다13,14. 협진이 시행되는 것에 대해 환자나 국민, 정책 입안자인 공무원은 비교적 긍정적인 편이지만 진료의 주체인 의사와 한의사는 실제 시행시 견해 차이가 있어 관련 내용과 절차에 관한 논의가 필요한 상황이다15-17.
본 증례에서는 의무기록을 통해 SAH의 위험인자라고 할 수 있는 고혈압, 당뇨병, 심장병, 뇌혈관질환 과거력을 조사하였다. SAH의 위험인자는 고혈압, 흡연, 과도한 알코올 섭취, 교감신경흥분제 섭취 등이며 흡연, 여성, 고혈압, 뇌혈관질환의 가족력이 있는 경우에는 다발성 동맥류의 위험도가 상승된다고 보고되었다. 당뇨병은 SAH의 위험인자로 보이지는 않는다고 하였다18. 본 증례의 과거력을 일반적인 위험인자와 비교해 보면 여성이 4명으로 비교적 많았다는 것 외에는 고혈압, 당뇨병, 심장병, 뇌혈관 질환 과거력 등에서 의미있는 결과로 보이는 것은 없었다.
SAH 발병시 발생하는 전형적인 증상은 활동 중에 갑자기 나타나는 매우 심한 두통, 일시적인 의식 소실, 뇌막자극 증상, 구토, 신경결손 등이다19. 본 증례 환자들의 SAH의 발생시 증상을 분석하면 5명 모두에서 두통이 있었으며, 4명에서 어지러움, 오심, 구토가 있었다. 두통 환자의 진료시 두통, 어지러움, 오심, 구토를 호소할 경우에는 두개내의 심각한 질환을 의심하고 적절한 진단과 관리를 해야 한다고 하겠다. 특히 벼락두통이 있을 경우에는 85% 정도에서 SAH와 관련이 있으므로 각별한 주의가 요망된다20. SAH로 인한 두통은 벼락 치듯이 갑자기 시작되어 병변 부위 쪽으로 나타나는 것이 일반적이며, 평생 처음 경험하는 듯한 심한 두통이 벼락치듯이 혹은 망치로 내려치는 듯하게 나타난다고 표현한다. 의식 저하 여부를 관찰해야 하며, 필요에 따라 뇌척수액 검사를 시행한다. 생명을 위협하는 적색 징후나 임상적 경고 기준이 없는 환자에서 촬영된 CT나 MRI는 신경학적으로 유의한 양상 진단이 나오는 경우가 드물다. 적색 징후나 경고 기준이 없는 경우의 CT나 MRI 촬영은 특별한 이상이 없다는 것을 확인하는 의미밖에는 없다21,22.
본 연구는 의무기록 조사에 의한 후향적 연구로 발병 당시 두통의 상세한 양상, 기타 발생 증상, 환자의 상세한 개인력 등을 확보하지 못한 점과 증례 환자 수가 적어 통계 분석 등을 수행하지 못한 것 등의 한계점이 있었다. 벼락두통 등 SAH가 의심되는 경우에는 비조영증강 CT 촬영이 필요하며, 한방의료기관에서 질환의 정확한 진단과 적절한 치료를 위한 협진 시스템의 개발과 CT 검사 적용 방안 마련이 필요하다고 하겠다.