치매의 침치료에 대한 해외 RCT 연구 동향 - pubmed의 2000~2018년 검색을 통하여 –
Recent RCT Research on the Effects of Acupuncture on Dementia - Based on a PubMed Search of Literature Published from 2000 to 2018
Article information
Abstract
Objective
The purpose of this study is to investigate recent clinical studies on the effects of acupuncture on dementia.
Method
We searched RCTs (randomized controlled trials) using the database PubMed (2000-2018). Clinical RCT studies of acupuncture used to treat dementia in humans were included. Nine randomized controlled trials were included.
Results
Various acupoints such as Baihui (GV20), Sishencong (EX-HN1), Fengchi (GB20), and Shenting (GV24) were used to treat symptoms. The studies reported a decrease in evaluation criteria, such as the Mini Mental State Examination (MMSE) and activities of daily living (ADL), for measuring cognitive ability. The acupuncture process, the results for outcome measure, and the effectiveness of studies were analyzed. We then assessed “risk of bias.”
Conclusions
Through this review, we found that acupuncture is applicable for the treatment of dementia. This can be used for future study.
I. 서 론
치매는(dementia)는 ‘후천적으로 획득된 인지기능 손상에 의해 성공적인 일상생활 수행이 불가능해진 상태’로 정의되며1, 대뇌반구 특히 대뇌피질(cortex) 및 해마(hippocampus)를 침범하는 미만성 질환(diffuse disease)에 나타나는 지능, 행동 및 성격 등의 점진적 황폐화(progressive deterioration)를 의미한다. 치매는 어떤 연령에도 나타날 수 있으나 특히 장년층 및 노년층에 더 빈번하며, 60대에 1%, 70대에 5%, 80대에 15%로 나이가 증가할수록 유병률이 증가한다2.
치매의 대표적인 원인으로는, 알츠하이머병, 혈관성 치매, 파킨슨병, 알코올 중독 및 약물 중독 등이 있다. 치매의 가장 흔한 원인으로 60%를 차지하는 것은, 콜린성 신경 소실에 의해 기억장애로 시작하여 언어와 시공간감각 결손으로 진행하는 퇴행성질환인 알츠하이머병이다. 알츠하이머병에서는 대뇌피질의 미만성 위축과 이차성의 뇌실확장이 관찰되며, A β아밀로이드를 함유한 신경돌기반(neuritic plaque)과 신경세포질 내의 염색되는 신경섬유원농축제(neurofibrillary tangles, NFTs)이 다량으로 관찰된다. 혈관성 치매가 20% 가량을 차지하여 두 번째로 흔한 원인이며, 크게 다발경색치매와 미만성의 백질 병변으로 나누어진다. 이 외에 파킨슨병과 연관된 루이소체치매가 10%, 픽병이 5% 가량을 차지하며 기타 흔하지 않은 원인으로는 구조적 질환, 감염, 영양성, 대사성, 외상 등이 있다1.
아직 완치법은 존재하지 않지만, 알츠하이머병에 의해 발생하는 행동, 신경학적 문제를 최대한 오랜 기간 동안 개선하기 위해 도네피질(donepezil), 리바스티그민(rivastigmine), 갈란타민(galantamine) 등이 미국 FDA에서 허가받은 치료제이며, 콜린분해효소를 억제해서 대뇌의 아세틸콜린의 농도를 증가시키는 기전으로 사용된다.
한의학에서는 역대로 痴呆를 呆痴, 愚痴, 文痴, 武痴, 呆病 등의 용어를 사용하여 왔으며, 선천적인 不足, 후천적인 정신자극, 노화로 인한 虛衰 및 他病에서의 轉變 등에서 나타날 수 있다고 하였다. 또한 先天稟賦不足과 後天調理失養으로 인한 인체의 생리적 작용이 저하되어 두뇌로의 영양공급이 저하된 本虛症(髓海不足, 肝腎精虧, 脾腎陽虛)의 바탕 위에 火, 痰, 瘀가 위로 淸竅, 腦絡의 정신기능을 손상시키는 標實證(瘀血內阻, 痰濁阻竅, 心肝火盛)의 挾雜에 의해 발생한다고 본다. 그 중 대표적으로 뇌의 만성적 진행성 변성질환에 의해 생기는 노인성 치매는 虛症의 경향이, 中風症狀과 연관되는 점을 관찰하여 일반적 痴呆와 다르게 인식된 혈관성치매는 實證의 경향이 조금씩 강할 수 있다. 그러나 모두 虛症을 근본으로 갖고 있던 사람에게 實證이 추가되어 일어나는 것이니, 本虛標實로 보아 침구치료로는 大椎 安眠 足三里瘂門內關神門靈都의 경혈로 치료하는 경우가 많다3.
치매의 한방치료에 관한 국내 연구를 살펴보면 2018년 3월 현재 증례보고 5편, 증례군 연구 6편, 실험연구 8편, 종설 8편으로 총 27편이 나와 있는 것으로 보이며(Table 1) 한약 치료, 통합 치료의 효과에 대한 연구는 밝혀져 있으나 국내 연구 실정상 침치료에 대한 대규모 연구가 진행된 바 없어, 외국의 사례를 수집하여 국내 연구의 기초 자료로 활용하고자 본 연구를 기획하였다.
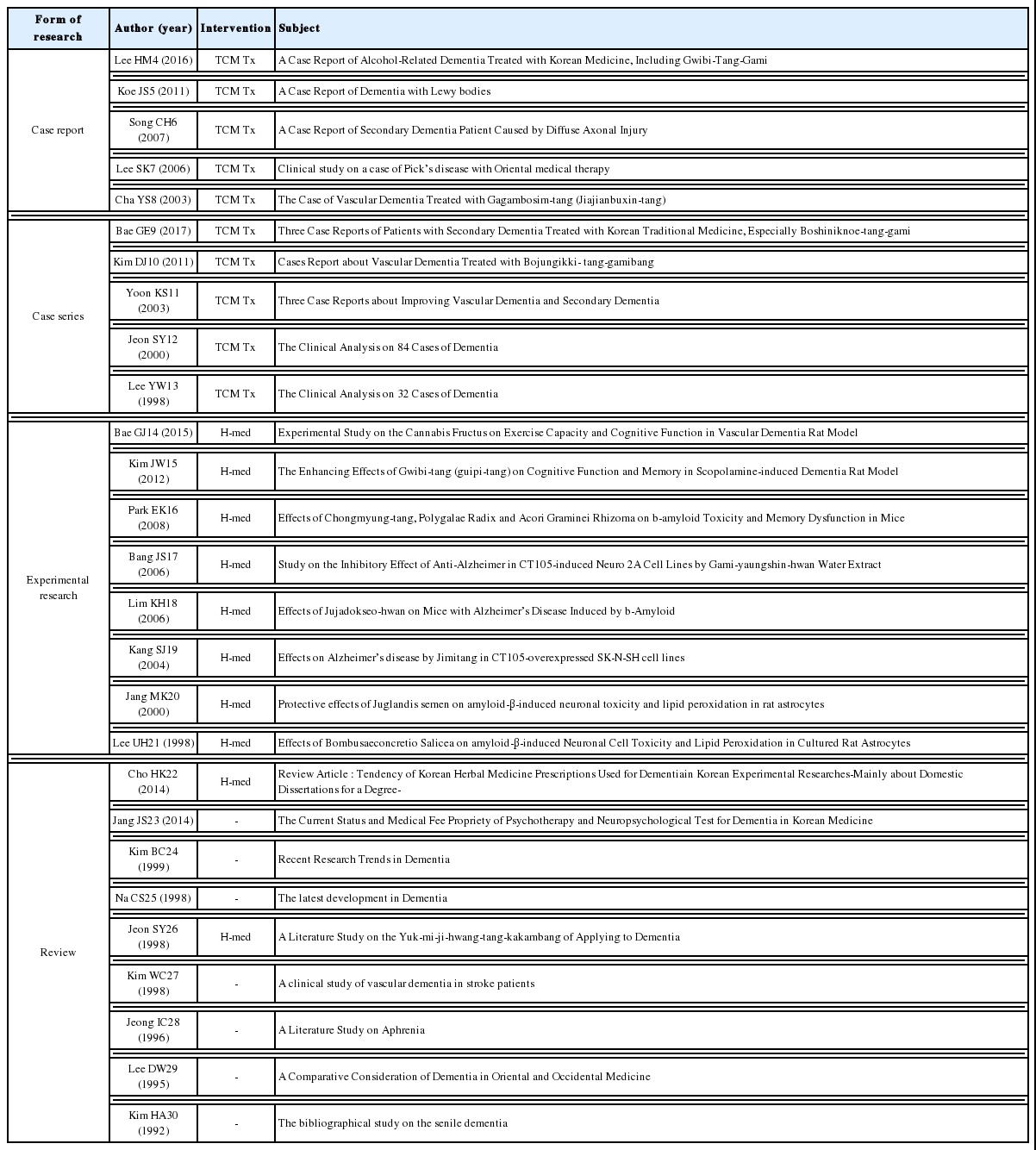
Published Year, Subject and Title of Journal of Domestic Research
II. 연구대상 및 방법
최신 연구 경향을 알아보기 위해 2018년 3월 1일 검색일을 기준으로 Pubmed에서 2000년 1월 1일에서 2018년 1월 1일까지의 논문을 검색하였다. 검색어는 dementia AND acupuncture로 한정하였으며, 사람 대상 연구 및 RCT 연구를 대상으로 하였다. 검색된 논문은 총 245편이었으며 1, 2차 screening에 의해 최종 9건의 논문이 선정되었다. 해당 내용은 PRISMA Flow diagram으로 나타내었다(Fig. 1).
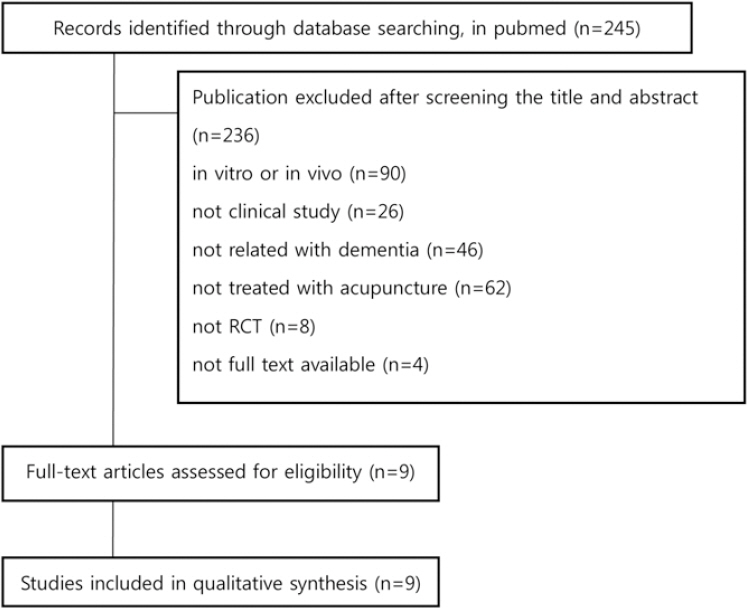
PRISMA flow chart.
III. 결 과
무작위 대조 연구 논문을 분석한 결과는 다음과 같다. 각각의 논문에 있어 진단 기준이 통일되지 않았고 치료 방법과 효과 평가 방법 또한 차이가 있어 무작위 대조 연구 논문의 실험군과 대조군 환자의 특징, 치료 방법, 환자군에 따른 치료 결과의 차이 등을 위주로 살펴보았다.
IV. 고 찰
치매는 뇌의 만성적 진행성 변성질환으로 흔히 기억장애 및 기타 지적 기능의 상실이 일어나는 임상 증후군이다. 치매는 일으키는 각종 질환에 따라 알츠하이머병(AD), 다발성 뇌경색 치매, 전두측두엽 치매, CADASIL 병, AIDS 치매복합, 대사성 치매, 정상뇌압 수두증, 외상, 뇌종양 등으로 분류할 수 있다. 각 질환의 출현빈도는 대상 연구 집단의 연령, 의료시설의 접근성, 출신 국가, 인종 또는 종족적 배경 등에 따라 달라지며, 특히 AD는 서양에서 치매의 가장 흔한 원인으로 치매 환자의 절반 이상을 차지하고 있다. 치매는 이들 개개 원인에 따라 진행 속도도 다르다. AD의 경우 치매는 수년에 걸쳐 매우 서서히 진행되며, 뇌염에 의한 치매는 수 주에 걸쳐 빠르게 진행된다. 또한 뇌혈관 질환에 의한 치매현상은 뇌졸중이 반복적으로 발생됨에 따라 점차 뚜렷해진다2.
한의학에서 치매는 ‘呆病’, ‘痴呆’ 등으로 분류하고 있으며 精氣不足, 脾腎虧虛, 痰濁阻竅, 氣滯血瘀, 氣血虛弱 등을 원인으로 보았으며, 阻氣鬱結, 逐其痰, 建其胃의 방법으로 治痰의 중요성을 언급하였다.
치매의 한방치료에 대한 국내 연구 동향을 살펴보면 증례보고 5편, 증례군 연구 6편, 실험연구 8편, 종설 8편으로 총 27편이었으나 침치료를 주된 치료법으로 시행한 경우는 없었다. 반면, Pubmed에서 검색한 해외 임상연구 결과를 살펴보면 치매의 침치료에 대한 RCT 연구와 문헌고찰 등이 다양하게 보고되어왔다.
본 연구에서는 9편의 RCT 연구 논문을 정리 및 분석하였다. 침 치료 이외에도 전침 치료, 양약 치료, 한약 치료, 재활 치료 등이 병행되었다. 치료혈위 분석 결과 총 9편의 연구에서 치매의 치료에 가장 많이 사용된 혈위는 百會(GV20)로 7편의 논문에서 사용되었고, 四神聰(EX-HN1)이 5회, 風池(GB20)가 5회, 神庭(GV24)이 4회 사용되었다. 百會(GV20)는 모든 맥이 다 모이는 곳이라는 뜻으로, 頭痛, 中風, 眩暈, 脫肛, 子宮出血, 痔疾,尾骨痛, 足心熱, 小兒驚氣에 쓰이며, 三才穴 중의 하나로 虛症의 전신질환을 主治한다. 四神聰(EX-HN1)은 百會에서 前後左右 각 1촌에 위치하는 4개의 혈로 頭風目眩, 狂亂風癎에 효과가 있다. 神庭(GV24)은 前頭痛, 目赤腫痛, 眼炎, 眼發赤, 鼻疾患를 主治하며 風池(GB20)은 中風七處穴 중의 하나로 後頭痛, 項痛, 感氣, 鼻炎, 耳聾, 耳鳴 등을 主治한다. 또한 논문에 사용된 치료 혈위를 가장 많이 포함하고 있는 경락은 督脈(7개), 足少陽膽經(5개), 足厥陰肝經(3개) 순으로 나타났다. 이는 督脈이 온 몸의 陽經을 통솔하며, 신경계 증상을 다루기 때문으로 사료된다. 또한 足少陽膽經은 인체의 燥濕寒熱風火의 六氣的 전체흐름 속에서 火에 관여하는 경락에 해당하는 것으로 手少陽三焦經과는 火의 발휘작용에서, 足厥陰肝經과는 風의 조절작용에서 연계성을 가진 역할을 한다. 이는 足少陽膽經이 눈, 귀, 협부의 병, 머리, 열병, 정신병을 치료하며, 表裏관계인 足厥陰肝經은 鬱滯된 氣를 순환하여 治痰을 우선하는 치매의 치법과 연관이 있기 때문으로 사료된다.
치료대상은 총 9편의 연구 중 혈관성 치매의 치료에 관한 연구가 7편, 알츠하이머성 치매의 치료에 대한 연구가 2편으로 나타났다.
대부분의 연구에서 침 치료의 효과가 우수한 것으로 나타났으나 침치료와 전침치료 간의 통계적 차이는 미미했다9 또한 실험군으로 침치료, 대조군으로 양약치료를 시행한 연구의 결과 평가 지표 점수의 큰 차이가 없었으며31,37이는 혈관성 치매와 알츠하이머 치매로 인한 각각의 연구에서 나타났다. 침 치료는 단독으로 행해지는 것뿐만 아니라 다른 치료와 병행되었을 때 더 효과적인 결과를 보였다32,33,35,38,39.
총 4건의 연구에서 adverse events에 대한 언급이 나타났다. Zhao Ling32의 연구에서 1명의 환자가 치료 3일째에 열이 동반되었지만, 전침 치료와 직접적인 연관은 없었다. Shi Gx35의 연구에서 25%의 환자군이 침 자극 부위의 불편감을 느꼈고, 20%의 환자들이 침자극 부위의 자반을 동반했다. Yujie J37 연구의 침치료 그룹에서는 5명의 불면증, 4명의 변비, 6명의 전립선 비대증, 2명의 관절염 증상이 뚜렷하게 개선된 예상치 못한 발견이 있었다. Shuhua W38의 연구에서 비정상적인 위장관 반응, 심혈관 반응, 알러지 반응이 동반된 경우가 있었으나, 치료와 명확한 관련성은 밝혀지지 않았다.
연구에서 효과를 판정하기 위한 평가지표는 MMSE, ADL, BDS, HDS, BBS, CNDR, DEMQOL, Picture recognition score, Clock drawing test, ADAS-cog, CIBIC-Plus, ADCS-ADL, NPI, MoCA score 등으로 나타났다. 이 중 가장 많이 사용된 지표는 MMSE로 7편의 연구에서 나타났고, ADL은 2편, 기타 지표는 1편에서 나타났다. MMSE는 간이 정신상태 검사로서 기질성 정신장애와 기능적 정신장애를 구별하며 인지기능 장애의 정도를 정량적으로 평가할 수 있다. 인지기능 장애를 평가하기 위한 MMSE의 검사항목으로는 지남력(Orientation), 기억등록(Registration), 기억회상(Recall), 주의집중(Concentration)과 계산능력(Calculation), 시공간 구성능력(Visuospatial function), 그리고 언어와 관련되는 능력(Language Function)들이 포함된다40. 대부분의 연구에서 MMSE를 사용한 반면, Shuhua W38의 연구에서는 MoCA score가 사용되었는데, 이는 MoCA가 경도인지장애의 평가에 더 민감한 도구로서 사용되었기 때문으로 보인다. 또한 Yujie J37의 연구에서 사용된 지표인 ADAS-cog, CIBIC-Plus, ADCS-ADL, NPI는 알츠하이머 환자에 대한 평가로서 사용된 것으로 보인다.
Cochrane의 Assesment of Risk of Bias(Table 4)에 따르면, 절반 가량의 연구에서 무작위 환자 배정을 하였다고 나와 있으나, 정확한 방법을 명시하지 않아 선택 비뚤림의 위험이 존재했다. 또한 침 치료와 양약 치료를 비교하는 연구가 많았지만, Placebo약이나 Sham침을 사용하였다고 명시된 경우가 없어 실행 비뚤림의 위험이 높았다. 결과 확인에 있어서는 결과평가에 대한 눈가림을 시행한 경우가 있었고, 눈가림 시행에 대한 여부를 명시하지 않은 연구도 존재했다. 탈락 비뚤림에서는 Per-protocol (PP) analysis를 이용하여 탈락 비뚤림이 높은 연구가 1건, 이외에 프로그램을 이용하여 결측치를 산정하거나, 결측치에 대한 언급이 없는 경우가 있었다. 또한 프로토콜이 없거나, 결과치가 누락되어 보고 비뚤림에 대해서 명확하게 평가할 수 없는 경우가 대다수였다. 대다수의 연구에서 명확한 눈가림이 시행되었는지, 결측치 산정이 어떻게 진행되었는지에 대한 언급이 불분명하여 한계를 보인 반면, 대다수의 항목에서 낮은 위험도를 나타낸 Yujie J37의 연구에서는 밀봉된 봉투에 의한 무작위 배정, 두 명의 눈가림된 평가자들에 의한 정보 수집, 통계 프로그램을 통한 결측치 산정, 프로토콜에 따른 결과 보고를 통해 낮은 비뚤림 위험도를 드러냈다. 그러나, 침치료군과 양약치료군에 대해 가능한 한 같은 치료를 받았다고는 나와 있으나 어떤 방법을 사용하였는지 명확하게 드러나지 않은 한계가 있었다.
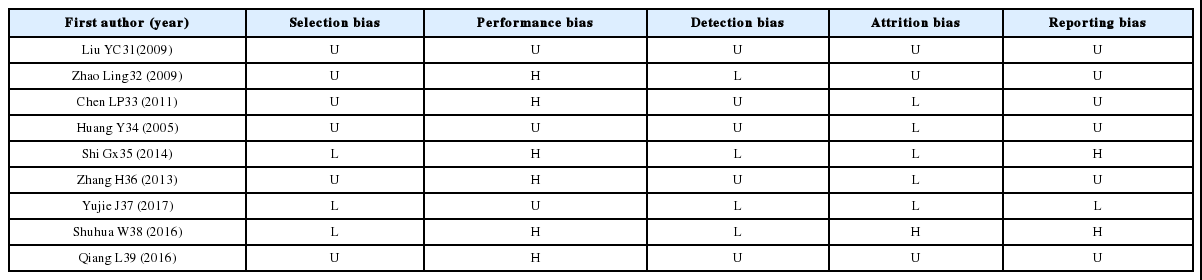
Assessment of Risk of Bias

Summary of Clincial Studies about Acupuncture for Dementia
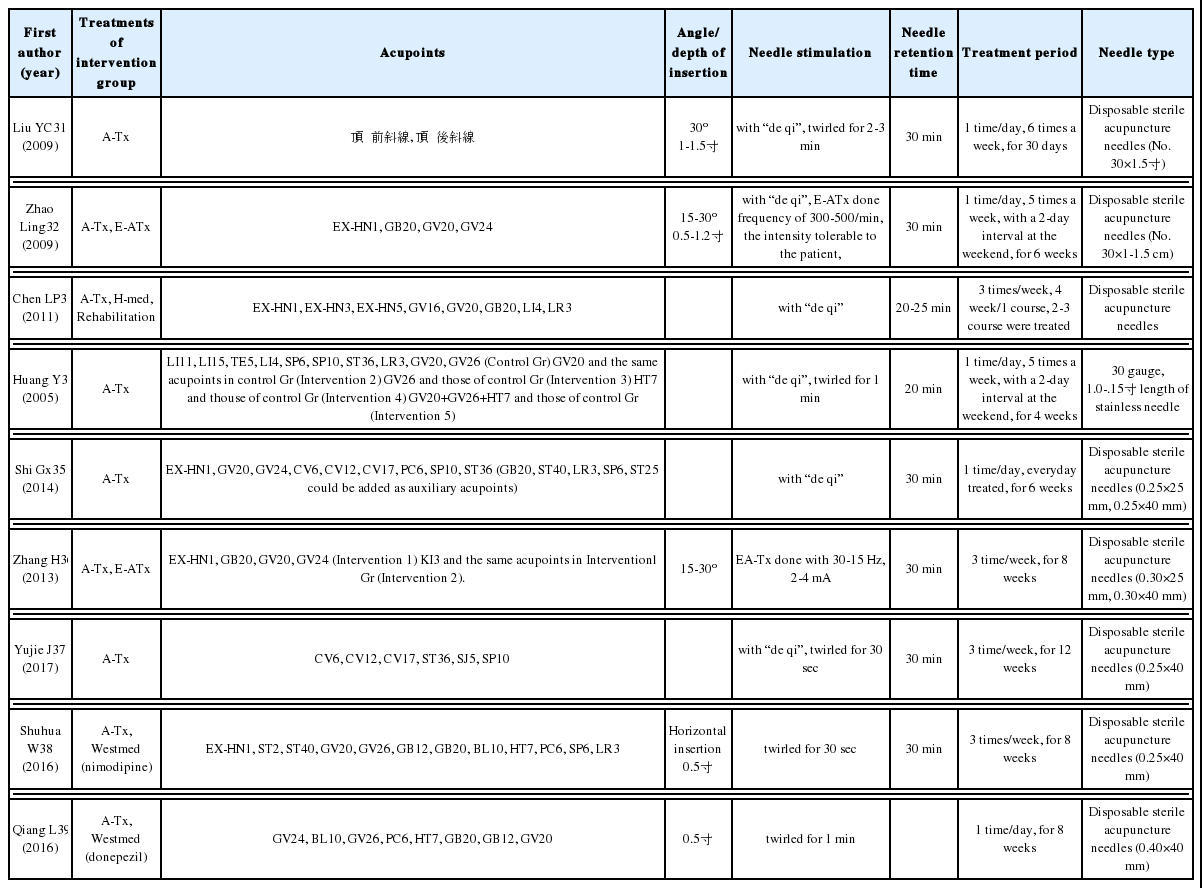
Process of Acupuncture for dementia
통계청에서 건강보험 자료를 이용한 2015년 한방에서의 질병 소분류별 입원 다빈도 상병 급여현황에서 알츠하이머병에서의 치매(F00, G30+-)는 13순위로 2014년(15위), 2013년(17위), 2012년(21순위)에 비해 연간 차지하는 비율이 높아지고 있다. 뿐만 아니라 World Alzheimer Report(2015)에 따르면 2017년 OECD 국가 평균 치매 환자 발병률은인구 1000명 당 연간 15명으로 2037년에는 인구 1000명 당 연간 25명까지 증가할 것으로 예상된다.
한국보건의료연구원에서 수행한 연구사업의 결과 보고서에 의하면 2005년 전 세계의 치매환자는 2,930만 명으로 추산되었고 치매로 인한 사회적 비용은 3,154억 달러에 이르는 것으로 추산되었다. 앞의 내용과 같이 치매의 침치료에 대한 연구가 국내외적으로 다양하게 이루어지고 있는 것으로 보이며, 다가오는 고령화 사회에 대비해서 보다 많은 환자들이 치매의 치료에 대해 관심을 보일 것으로 보인다. 이에 한방 의료기관에서 치매로 내원한 환자들에 대하여 기존의 치료와 함께 침치료를 적극적으로 사용하게 된다면 증상 진행의 완화에 보다 도움을 줄 것으로 사료된다.
본 연구에서 선정된 RCT 연구들은 다수의 환자들을 대상으로 대규모 연구로 진행되었으며 국내의 치매 관련 한의학 연구에서 치험례와 실험연구 위주로 진행된 것에 대해 그 연구의 수와 규모 면에서 매우 큰 차이가 있다. 본 연구에서는 RCT 위주의 논문을 살펴봄으로써 문헌 검색 범위가 좁은 한계가 있었으며, 몇몇 논문에서 통계적 유의성과 부작용에 대한 언급이 부족해 메타분석이 어려운 점이 있었으며, 추후 이러한 점을 보안한 높은 수준의 연구가 진행되어야 할 것으로 사료된다.