Well-Managed Myelodysplastic Syndrome Patients Treated with Traditional Korean Medicine; Report of Two Cases
한방 치료를 통한 골수이형성증후군 치험례 2례
Article information
Abstract
본 증례에서는 한방치료를 받은 두 명의 골수이형성증후군 환자를 통하여 골수이형성증후군에 대한 한방치료의 효과를 보여주고자 하였다. 골수이형성증후군은 골수의 증식과 구성 세포들의 이형성, 비효율적인 조혈을 특징으로 하는 골수의 악성 종양이다. 현재까지 골수이형성증후군에 대한 완벽한 치료법은 없으며 골수이형성증후군의 증상을 경감시키거나 급성 골수성 백혈병으로의 진행을 막는 목적으로 치료가 이뤄지고 있다. 첫 번째 환자는 1차성 골수이형성증후군 환자로 2011년 1월부터 2016년 현재까지 꾸준히 침 치료 및 한약치료를 받고 있다. 두 번째 환자는 난소암 치료를 위한 항암화학요법의 부작용으로 생긴 2차성 골수이형성증후군 환자로 2010년 10월부터 4년간 꾸준한 한약 복용 및 3번의 입원치료를 받은 환자이다. 침 치료, 한약 치료와 함께 환자들의 상태를 평가하기 위해 정기적인 혈액검사가 이루어졌다. 골수이형성증후군 진단 후 두 달에 한 번씩 수혈을 받으며 수혈 의존 경향을 보이던 첫 번째 환자는 한방치료 후 단 두 번의 수혈밖에 받지 않았고 급성골수성백혈병으로 진행하지도 않았으며 건강한 몸 상태를 유지하고 있다. 두 번째 환자 역시 꾸준한 한방치료를 통해 비교적 좋은 삶의 질을 유지하며 기본 체력 또한 많이 상승되면서 골수 이식을 받을 정도까지 몸 상태가 개선되었다. 본 증례보고는 마땅한 치료법이 없는 골수이형성증후군 환자들에게 한방 치료가 특별한 부작용 없이 환자들이 호소하는 증상을 개선하고 기본적인 체력 증진에 도움이 되며 급성 골수성 백혈병으로의 진행을 예방하는 동시에 기존의 보존적 치료법의 효과를 극대화 시키는 효과가 있음을 보여주는 증례라고 하겠다.
Trans Abstract
Myelodysplastic syndrome (MDS) is a typical myeloid malignancy characterized by cell dysplasia in bone marrow. Currently, there is no therapeutic treatment for MDS. The only available therapies either relieve symptoms or prevent the development of acute myeloid leukemia (AML). This study aimed to report the effects of traditional Korean medicine (TKM) on MDS by presenting two case reports. The patient in Case 1 was diagnosed with primary MDS and regularly received acupuncture treatments and herbal medicine. In Case 2, a patient with ovarian cancer was diagnosed with secondary MDS, which resulted from an adverse reaction to chemotherapy. This patient took herbal medicine for four years and was hospitalized three times. In order to have their condition evaluated, both patients underwent regular blood tests. The patient in Case 1, who showed blood transfusion dependency, received only two blood transfusions after TKM treatment, and the person’s health condition was stable as of January 2016 without any signs of AML development. The patient in Case 2 also has stable health condition. TKM treatment effectively treated their MDS symptoms and improved their general health conditions without any adverse effects. It also prevented the rapid development of AML and maximized the effects of conservative therapy.
I. Introduction
Myelodysplastic syndrome (MDS) is a typical myeloid malignancy characterized by cell dysplasia in bone marrow and inefficient hematopoiesis. The pathology of MDS is marked by a decrease in red blood cells (RBC) and bi-/pancytopenia1. The most common clinical signs and symptoms of MDS include fatigue, palpitations, shortness of breath, infections, and bleeding2.
The main etiological factors of MDS are non-specific. But as the people were getting older, the incidence rate of MDS was also increasing particularly over 65 years old in Korean people3. MDS can develop as a result of the adverse effects of radiation or chemotherapy, especially in younger populations4,5. Five-year relatively survival rate of MDS was 44.0% in 2008-2012 year in Korea3. A previous study demonstrated that approximately 20-25% of MDS patients have a risk of developing acute myeloid leukemia (AML)6.
Most patients with MDS undergo Western medical treatments, nevertheless, the effects of which remain unclear. Additionally, recent studies show that some adverse effects have appeared during Western medical treatments for MDS7. Currently, the primary medical treatments are focused on minimizing complications, relieving MDS symptoms, and preventing or delaying the development of AML in the hopes that patients will lead a normal life8.
There were plenty of reports about MDS in Western Medicine but there was only one case report about MDS patient in the field of Traditional Korean Medicine (TKM) in Korea9. This is a second case study about MDS patient treated with TKM.
This study aims to report the effects of TKM on MDS and intend to introduce the possibility of TKM on MDS in the field of TKM. In this study, we examine two cases of MDS, one with primary and the other with secondary MDS. In both cases, the patients were successfully treated with TKM treatment and did not show progression to AML.
II. Case report
<Case 1>
A 53-year-old woman with no special medical history and family history was referred to our institution in January 2011. In July 2010, the patient was diagnosed with primary MDS by a Western medical hospital. Bone marrow examination was conducted and genetic analysis showed that the patient had an extra eighth chromosome (trisomy 8), which is commonly observed in MDS patients (Fig. 1). After examination, she was considered to have refractory cytopenia with multilineage dysplasia (RCMD) according to the WHO classification.
Chromosome analysis of patient in case 1.
The patient have an extra eighth chromosome (46, XX, +8).
The patient showed classic signs of MDS such as anemia and transfusion-dependency. After diagnosis of MDS in July 2010, the patient received transfusion therapy every two months before starting TKM treatment by Western medical hospital. Regular blood tests were performed approximately every four weeks until April 2012. As the patient’s condition became stable, the interval between each blood test was increased (Table 1).
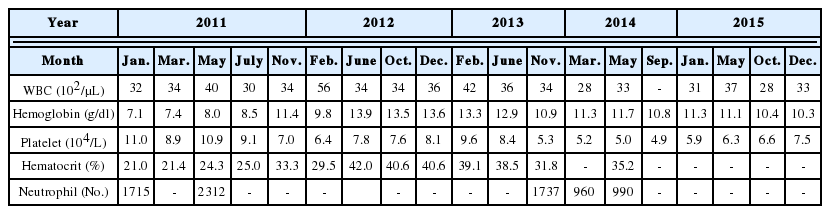
The Serial Change of Hematological Analysis from Patient in Case 1
Until recently, the patient visited our institution regularly for acupuncture treatment two to three times a week from January 2011. Conventional Western medical treatment was not performed. Only acupuncture treatment was performed; hospitalized treatment was not performed. The following were the patient’s primary signs and symptoms: lassitude, edema, dizziness, and bleeding gums. Depending on the severity of these signs and symptoms, we administered acupuncture at various specific acupuncture points that were chosen according to Sang-Su theory. Sang-Su theory is a theory involving Asian image-mathematics based on the I-ching. Asian image-mathematics is also one of the ways to explain the Yin/Yang &Five elements theories that are the basis of TKM10. We selected acupuncture points according to our diagnosis and monitored the patient’s condition. Acupuncture points of Foot’s Minor Yin Kidney Meridian (足少陰腎經) were considered as main Meridian improving hematopoiesis of bone marrow and symptoms of patient (Table 2).

Acupuncture points for Each Patient
In March 2011, an herbal medicine regimen was recommended in order to work synergistically with the acupuncture treatments. For the first time, Sibjeondaebo-tang-gami (SDTG) (Table 3) was prescribed, and the patient was advised to take it twice daily for one year. SDTG is composed of sibjeondaebo-tang with the addition of Cervi Pantotrichum Cornu. Sibjeondaebo-tang is frequently prescribed in TKM for patients who are deficient in Yang-Qi and Blood, have a chronically poor health condition, lack of appetite, or are suffering from exhaustion11. In TKM, Cervi Pantotrichum Cornu invigorates Qi and Blood and is often prescribed for anemia due to its hematopoietic effects12.

Prescription of Sibjeondaebo-tang-gami (SDTG)
General condition of patients grew much better and the regular RBC transfusion had not been done since the patient started to receive TKM treatment in January 2011. However, the RBC transfusion was done in May 2011 only one time because the patient’s physical condition was so bad with a great deal of fatigue, dizziness, and lassitude.
Over the course of a year of TKM treatment, the patient’s signs and symptoms, including shortness of breath, bleeding gums, and lassitude, were notably improved and her general condition remained relatively stable. Since March 2012, the patient has not taken any herbal medicine and received only acupuncture treatments.
In November 2013, the patient suffered from acute abdominal pain and was diagnosed with ileocolitis. The patient underwent Western medical treatment for the following two weeks. An RBC transfusion was performed for the first time since May 2011. Since the last RBC transfusion in November 2013, no additional blood transfusions were performed, and her health condition has been well maintained over 5 years through February 2016.
<Case 2>
In October 2010, a 50-year-old woman with ovarian cancer was referred to our institution for MDS treatment. The patient was diagnosed with secondary MDS, which resulted from an adverse reaction to chemotherapy.
Prior to her first visit, the patient had been diagnosed with ovarian cancer in June 2001, and had undergone two operations in June and October 2001. Following the operations, the patient received six sessions of chemotherapy. Follow-up studies were done regularly, but recurrent carcinoma was found in April 2008. The patient received nine additional sessions of chemotherapy in 2008. Besides ovarian cancer, the patient had no previous medical history and family history.
The patient was diagnosed with RCMD type MDS in October 2010. Examination of the patient’s bone marrow revealed monosomy 7, a common cytogenetic finding in patients with MDS (Fig. 2). The blood levels at diagnosis are shown in Table 4.
Chromosome analysis of patient in case 2.
The absence of seventh chromosome is observed (46, XX, -7).
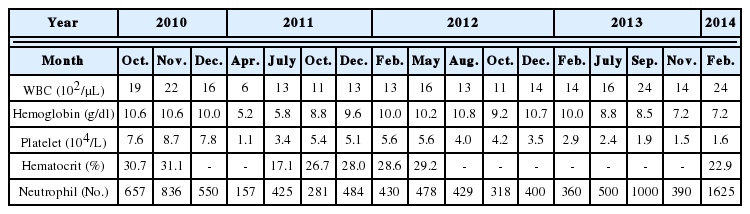
The Serial Change of Hematological Analysis from Patient in Case 2
The patient was admitted to our institution for 19 days in November 2010. Prior to admission, the patient’s only Western medical treatment was a folic acid prescription; no other biomedical treatments were performed. At our institution, the patient received TKM treatments, including acupuncture, twice daily. The patient was prescribed the same SDTG formula as the Case 1 patient (Table 3). SDTG is an herbal formula representative of TKM and usually used for the patients who are Qi and Blood deficient. The patient took SDTG three times daily. Based on TKM theory, especially Sang-Su theory10, we selected several acupuncture points, and acupuncture was performed relevant to the patient’s condition. Acupuncture points of Foot’s Minor Yin Kidney Meridian (足少陰腎經) and Foot’s Major Yin Spleen Meridian (足太陰脾經) were selected mainly (Table 2).
In December 2010, the patient received chemotherapy for MDS; the drug administered was azacitidine, a well-known treatment for MDS in Western medicine. While the patient was being treated with azacitidine, she was admitted to an isolated intensive care unit and RBC transfusion was performed due to severe pancytopenia. During platelet transfusion, the patient suffered from anaphylactic shock, and so the azacitidine chemotherapy could not be completed. Importantly, the patient was neither taking herbal medicine nor visiting our institution during the four sessions of chemotherapy.
The patient returned to our institution in June 2011 to begin taking herbal medicine. Although outpatient treatments were rarely performed, the patient had been regularly taking the medicine twice a day until next hospitalization. Her overall condition was fairly well maintained after taking herbal medicine.
The patient was admitted to our institution for the second time in November 2013 for a period of 26 days. During this time, the patient regularly took herbal medicines, including a slightly modified SDTG, three times daily, and acupuncture treatment was performed twice daily. The patient’s third admission was in February 2014 for 20 days. The herbal prescription was the same as the one from the second admission. After discharge the patient had taken herbal medicine until June 2014.
Over the course of four years of TKM treatment, from November 2010 to June 2014, the patient received continuous herbal medicine treatments with SDTG, Guibi-tang, Hang-am-dan, etc. Guibi-tang is also one of the frequently prescribed herbal formula in TKM treatment for who are suffering from fatigue, palpitation, insomnia, Qi and Blood deficiency. Hang-am-dan is the herbal formula which has anti-cancer effect13. SDTG was the most frequently prescribed formula for Case 2 patient; however, depending on the patient’s signs and symptoms, other herbal elements were either added or removed to the formula while maintaining its basic composition.
III. Discussion
Most patients with MDS are frail, elderly, and suffering from comorbidities14. Moreover, bleeding and various infections are major causes of death in MDS patients. Progression of MDS patients to the AML stage is mainly characterized by death15.
For MDS patients without any particular symptoms, the wait-and-see prescription is recommended. Clear treatment methods are not known for either high-risk MDS patients or patients suffering from serious cytopenias2,8.
Currently, no treatment options result in a complete recovery from MDS. Several study groups have tried to treat MDS using Western methods, but these methods are limited in that they are often expensive with unclear efficacies. Furthermore, current treatments only focus on relieving MDS symptoms and preventing or delaying progression to the AML stage.
We dealt with two patients diagnosed with RCMD type MDS: one patient with primary MDS and the other with secondary. RCMD-type MDS is observed in up to 24% of all MDS cases, and the average life expectancy is roughly 30 months7,16. In WHO-based Prognostic Scoring System (WPSS) which is one of the prognostic systems for MDS, both patients were classified into the high-risk group with score 3. The average life span of high-risk group marks around 2 years and 54-63% of them are mostly likely to progress to AML within 5 years17.
Both patients continually received TKM treatment over 4 years. Especially patient in Case 1 took herbal medicine about 1 year and has received acupuncture treatment until now 2 to 3 times a week. Patient in Case 2 took herbal medicine about 4 years and was hospitalized 3 times total of 65 days. As they received TKM treatment, they have survived more than 5 years. It’s longer than average life expectancy of high-risk RCMD type MDS patients. Moreover they had relatively stable health conditions and never developed AML.
The patient in Case 1 underwent an RBC transfusion every two months after diagnosis of MDS in July 2010 and showed transfusion-dependency. As referred to in a previous study, transfusion- dependent patients are more likely to progress to AML and have a lower survival rate than those who are not transfusion-dependent. The average life span of transfusion-dependent patients is 10.74 months and is higher for transfusion-independent patients at 23.83 months18. The patient received TKM treatment and underwent only two blood transfusions. The first transfusion was in May 2011 when she initially started receiving TKM treatment; the latter was in November 2013 when she was treated for acute ileocolitis. Since then, only TKM treatments have been performed. Although one can argue that the blood test results (Table 1) show both improvement and deterioration, the patient never developed AML and maintained a relatively healthy and stable condition up to date.
The patient in Case 2 was diagnosed with secondary MDS. Generally, secondary MDS not only tends to have a worse prognosis than primary MDS, but also does not respond as well to treatment. At the time of diagnosis, both conservative treatment and chemotherapy with azacitidine were required and performed. However, wait-and-see therapy was the only course of action for the patient due to the failure of azacitidine therapy. The patient voluntarily chose to undergo TKM treatment. Although the blood test results occasionally varied, it was observed that undergoing TKM treatment for a long period of time had helped to stabilize the patient’s condition enough for a bone marrow transplant.
As seen above, TKM treatments utilizing acupuncture and herbal medicine have effectively helped patients with MDS by reducing their symptoms and improving their general condition. Our present study was limited in that we could not adequately provide the impressive data of the two MDS cases, because MDS therapies are primarily focused on relieving its related symptoms. In addition, because this study is a case report, clearly stating the causal relationships between acupuncture and herbal medicine and determining which is more effective for the treatment of MDS is difficult. However, both patients continuously received TKM treatment, which led to a reduction in their MDS symptoms. Moreover, our treatments successfully improved the quality of life for both patients and prevented the rapid development of AML. Presently, no perfect MDS treatment exists in Western medicine. Although TKM does not completely cure MDS, acupuncture and herbal medicine are therapeutic options for MDS patients.
In summary, we suggest that TKM treatments are able to help patients with MDS, but more effective therapies will need to be developed. Furthermore, we expect that an interdisciplinary approach that combines TKM and Western medicine will be beneficial in developing an effective treatment approach for MDS. We also hope that this report acts as a starting point for the active use of TKM for patients with MDS.
Acknowledgement
This study was supported by the Association of Sang-Su Medicine (ASSM) which is one of the Traditional Korean Medicine study groups in South of Korea.