





I. Introduction
Functional dyspepsia (FD) is one of most common disorders in gastrointestinal (GI) system, as the estimated prevalence of 10% to 30% worldwide and 8 to 37 % in Korea1-3. It refers to the recurrent or persistent dyspeptic symptoms more than 6 months without explainable organic causes4. Accordingly, the diagnosis of FD is made by the self-report-based feature of symptoms called ‘Rome IV Criteria for functional criteria’5. FD is known as a multi-causal disorder, which infection of Helicobacter pylori, visceral hypersensitivity, low-grade mucosal inflammation, and/or delayed gastric emptying are involved in its pathophysiology6.
FD patients have a poor quality of life (QoL) more than those with other GI functional disorders including gastroesophageal reflux or irritable bowel syndrome7. In general, proton pump inhibitors (PPI), selective serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants (TCA) or prokinetic drugs are used for treatments of FD8. FD has the highly complex pathologies, which induce these conventional therapies to have limitations such as lower response and frequent relapse after cessation9. Accordingly, many clinicians and patients are looking for herbal remedies in an aspect of multi-targeted medicine10. For example, Banhasasim-tang (半夏瀉心湯) and Yukgunja-tang (六君子湯), two popular herbal prescriptions had shown the clinical efficacy on FD patients11,12.
On the other hand, a quarter of patients has a refractory FD characterized by a long duration, severe symptoms, and poor QoL in spite of medical treatment13. These refractory FD patients are particularly problematic, and many alternative approaches including electroacupuncture have been tried to manage them14. In addition, a patient-customized herbal therapy is recommended for these patients.
This study reports a severe case of refractory FD who showed a rapid response to an Nangan-jeon (暖肝煎) decoction. Nangan-jeon a formula for ‘cold symptoms of the liver- and kidney-Yin (肝腎虛寒), then no study exist for the ant-FD therapeutic effect yet.
II. Report of the case
1. Characteristics of patient and medical history
A 61-year-old woman has been suffering from persisting postprandial fullness, early satiation after meal and sometimes epigastric pain since her teenage. The symptoms have used to restrict her food life and to worsen daily life frequently. She had been diagnosed as functional dyspepsia long before visiting author’ clinic, based on non-specific finding from gastroscopy multiple times. The patient frequently had visited Western clinics and took various conventional drugs (prokinetics, PPI or SSRIs) when she felt the bad condition. However, her symptoms had been repeated the a little better and worsen again. From April 2020, the patient felt the worse dyspepsia-related symptoms after hard exercise and heavy sweating over.
The patient was generally susceptible to cold and psychological stress, and no change of body weight with around 19.0 of body-mass index (height 157 cm, body weight 47 kg). She had no specific family history, but had a diagnosis of Raynaud’s disease in her 20s. The patient thus has tried to physical exercise intentionally, and has neither used alcohol, smoking and drugs, nor had food-allergic reaction.
This case study was approved by the institutional review board (IRB) at Daejeon Korean Medicine Hospital (IRB number: DJDSKH-21-E-14-1).
2. Diagnosis, treatments, and course of symptom
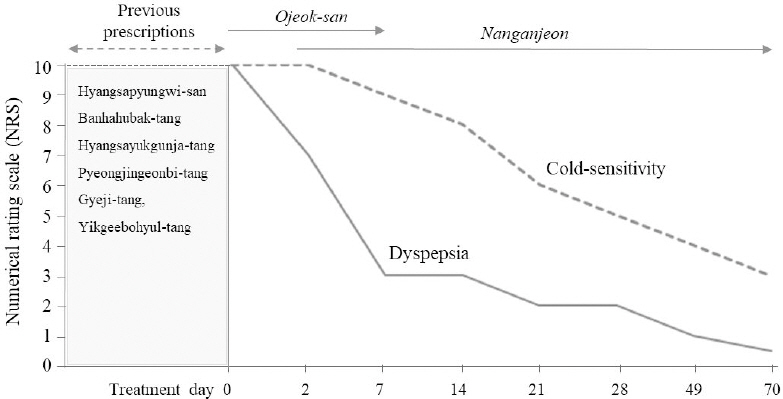
Her abdominal discomfort including postprandial fullness, gastric satiation and especially severe epigastric pain became worse from one year, while these symptoms were affected by eating meals and worsened under cold circumstance. Her complaints weren’t better even various treatments from both Western and Korean medicine clinics, and thus she was transferred to author’ clinic on January 2021. As expected, her symptoms met the Rome IV Criteria for functional criteria14 (Table 1). On September 2020, the patient started to be treated in other department of same hospital for about four months, but not much improved even six different herbal decoctions, Hyangsapyungwi-san (香砂平胃散), Hyangsayukgunja-tang (香砂六君子湯), Banhahubak-tang (半夏厚朴湯), Pyeongjingeonbi-tang (平陳健脾湯), Gyeji-tang (桂枝湯) and Yikgeebohyul-tang (益氣補血湯), respectively.
Table 1
Rome IV Criteria for Functional Criteria
Author examined her history and characteristics of clinical symptoms, while she had a mild white-color coat at tong and rapid-weak pulsation. The patient fell into Soumin of Sasang constitutional classification using QSCCII. Author thought the cold-derived dyspepsia based on the pattern identifications of “liver-kidney deficiency cold (肝腎虛寒)”. Author tried to test the response to Ojeok-san (五積散), and then confirmed the quick positive effect. The self-reporting NRS score (0 means no symptom while 10 doses the worst severity15) was quickly decreased from NRS 10 to NRS 7 in 2 days. This positive response gave author the convincing diagnosis of “Liver-Kidney Deficiency Cold” which decided to prescribe Nangan-jeon (Table 2). This herbal drug rapidly improved her overall dyspeptic symptoms, into NRS 5 (after 1 week) and NRS 2 (after 3 weeks) followed by normal level of digestive function (NRS 1) after 7-week treatment, respectively (Fig. 1). In addition, her cold-sensitivity also decreased by NRS 5 on 4-week and gradually became better in length of taking Nangan-jeon (Fig. 1). In fact, acupuncture (CV12, HT7, LI4, SP4, SP6, ST36), moxibustion (CV4, KI1) and Aconitum pharmacopuncture (CV4 and BL23) were also given to her, as twice weekly for one month and followed by once per week later, respectively. As expected, her mild white-color coat at tong was changed into a bright-color and the rapid-weak pulsation also a little improved.
Table 2
Composition of Nangan-jeon
| Scientific name | Herbal name | Chinese name | Dose* |
|---|---|---|---|
| Lycium chinense Miller | Lycii Fructus | 枸杞子 | 24.0 g |
| Angelica gigas Nakai | Angelicae Gigantis Radix | 當 歸 | 16.0 g |
| Poria cocos Wolf | Poria Sclerotium | 白茯苓 | 16.0 g |
| Foeniculum vulgare Miller | Foeniculi Fructus | 小茴香 | 16.0 g |
| Lindera strichnifolia Fernandez-Villar | Linderae Radix | 烏 藥 | 16.0 g |
| Cinnamomum cassia Presl | Cinnamomi Cortex | 肉 桂 | 8.0 g |
| Aquilaria agallocha Roxburgh | Aquilariae Agallochae Lignum Resinatum | 沈 香 | 4.0 g |
III. Discussion and Conclusion
FD is known to show the epidemiologic features of a 1.4 to 2.7-fold female predominance along with a lower QoL than men16. Author also found a higher prevalence of FD in females by approximately 2-folds (14.2% of male versus 26.9% in female)17. In addition, females were known to poorly respond in FD by H. pylori eradication, one of main treatments for FD18. A clinical data using 1,341 Chinese FD patients presented 24.4% of the refractory FD, and a tendency of female-predominance (male 22.9% versus 25.4%)12. In general, we call refractory FD if symptoms are unresponsive to at least two medical treatments, such as acid suppressors, proton pump inhibitors, or prokinetics, for six months19.
The patient of this case report showed a typical refractory FD pattern because both previous conventional and herbal drugs didn’t work efficiently. In aspect of the subtypes of FD, this patient showed the overlapping feature of postprandial distress syndrome (PDS) and epigastric pain syndrome (EPS). In a Korean study, the proportion of PDS and EPS were 53.6% and 31.8%, while 14.6% of FD belonged to the PDS plus EPS20. One clinical study revealed the preference of the EPS+PDS subtype in patients with refractory FD than in patients with non-refractory FD12.
This study assessed the improvement of symptoms using self-reported NRS score, then her most of signs including postprandial fullness and notable epigastric pain rapidly decreased. The previously prescribed herbal decoctions, Hyangsapyungwi-san, Hyangsayukgunja-tang, Banhahubak-tang, and Pyeongjingeonbi-tang, are generally used for FD, while some have been proven for their anti-FD efficacy from clinical studies21,22. This patient was however refractory to these decoctions. In Korean medicine, FD can be generally classified into 6 different pattern identifications such as ‘spleen and stomach deficiency and cold’, ‘liver-stomach disharmony’, ‘spleen deficiency with qi stagnation’, ‘tangled cold and heat’, ‘dampness and heat in the spleen and stomach systems’ or ‘food retention disorder’23. Then, ‘liver-kidney deficiency cold’, the patient’ pattern identification was not included.
In fact, the choose of the Nangan-jeon was made by the rapid response to Ojeok-san. Ojeok-san usually treats the pain-related disorders, but it has also the pharmacological action on the ‘cold’-related dyspepsia. In previous department, other two decoctions (Gyeji-tang and Yikgeebohyul-tang) targeting each the ‘cold’-related symptoms and ‘deficiency of qi and blood’ weren’t effective unlikely Nangan-jeon. Nangan-jeon first appeared in Gyeongakjeonseo(景岳全書), as a formula for ‘cold symptoms of the liver- and kidney-Yin’24. This formula showed the pharmaceutical properties to improve the female-fertility, under situations of especially ‘liver-kidney cold type’25,26, which supported the rationale to choose Nangan-jeon this woman patient. As ‘cold’-focused treatments were added using electronic moxibustion (CV4, KI1) and Aconitum pharmacopuncture (CV4 and BL23), as well as Soumin-related acupuncture (CV12, HT7, LI4, SP4, SP6, ST36), respectively. Aconitum was reported to exhibit a warming effect on the abdominal region such as CV12 and CV827, accordingly these treatments together might contribute to the improvement of this case.
To date, many approaches including electroacupuncture and psychiatric management using a tricyclic antidepressant have been tried to solve the refractory FD, but many limitations are still existing28,29. In summary, even this is only a case, Nangan-jeon-based therapeutics could be a fine choice for refractory FD. Of course, further studies are required to verify the therapeutic effects of Nangan-jeon and the proper applicable type of refractory FD.


