미세먼지 관련 호흡기질환 임상연구 동향
Abstract
Objectives:
This study aimed to review the clinical research trends in respiratory diseases related to particulate matter (PM) to help design clinical studies on herbal medicine that protects against PM.
Methods:
We searched three international databases (Pubmed, EMBASE, and CENTRAL) to investigate clinical studies on respiratory diseases related to PM and to analyze their study design, respiratory-related disease, inclusion/exclusion criteria, study period, outcome measure, study results, measurement method of PM and range of PM.
Results:
A total of 18 studies were finally selected, including 13 observational studies and 5 randomized controlled trials. The selected studies showed an increasing trend from 1985 to 2018 and were conducted mostly in North America, followed by Europe and Asia. Subject disease and age were decided in variety by each study objective, although asthma accounted for the majority. For the outcome assessment, pulmonary function test was mostly used for lung function. Quality of life questionnaires and biomarkers in blood and sputum were also used.
Conclusion:
A well-designed clinical study on herbal medicine that protects against PM is needed, and this study is expected to be used as base data.
Keywords: particulate matter, respiratory disease, clinical studies, herbal medicine
I. 서 론
대기오염으로 인한 사회적⋅경제적 문제 및 인체유해 영향에 대한 심각성이 제기되면서 전 세계적으로 대기오염에 대한 관심이 늘어나고 있다. 경제협력개발기구(OECD)에 따르면 대기오염으로 인한 전 세계 조기사망자수가 2010년 300만 명에서 2060년 600~900만 명으로 증가할 것으로 보고되었으며, 우리나라의 경우 이로 인한 조기사망자수가 2010년 359명에서 2060년에는 1,109명으로 급증할 것으로 예상되고 있어 1 이에 따른 추가대응이 필수적인 상황이다. 대기오염 물질 중 미세먼지가 최근 건강을 위협하는 가장 심각한 물질로 인식되고 있으며 2 우리나라 정부에서도 이에 따른 미세먼지 종합대책을 국정과제로 지정하여 2014년에는 169억 원, 2015년 179억 원, 2016년 3,881억 원, 2017년 4,834억 원의 사업비를 책정하여 다각도로 대책 방안을 추진하고 있다 3. 미세먼지는 공기 중의 총 부유분진(TSP, Total Suspended Particles) 중 직경 10 μm 이하의 먼지(PM, particulate matter)로 정의되며, 지름이 10 μm보다 작은 미세먼지(PM 10)와 지름이 2.5 μm보다 작은 초미세먼지(PM 2.5)로 나뉜다 4. 미세먼지가 발생한 지역이나 계절, 기상조건 등에 따라 입자의 크기와 구성은 다양하지만 5, 일반적으로는 황산염, 질산염, 탄소류, 광물 등으로 구성된다 6. 미세먼지는 입자의 크기가 매우 작아 인체 내로 더 깊숙이 침투하여 다양한 인체 내 염증반응을 일으키며 7 사망률의 증가, 심혈관계 영향, 호흡기계 영향, 암 발병률 증가 등에 대한 관련성이 여러 미세먼지의 건강유해평가 연구들에서 보고되었다 8. 이러한 위험 때문에 2013년 세계보건기구(WHO) 산하 국제암연구소(IARC)는 대기오염물질 가운데 미세먼지를 1급 발암물질로 지정하여 권고 기준을 두고 있다 9. 특히 호흡기계와 관련하여 미세먼지는 하부 기관지 및 폐 실질까지 침착되어 폐기능 감소, 만성폐쇄성폐질환(COPD, chronic obstructive pulmonary disease), 천식 및 폐암환자 발생 증가, 하기도 및 호흡기계 증상 증가 등을 초래한다고 발표되었으며 10, 미세먼지가 활성산소 생성을 증가시켜 염증 반응을 유발시킨다는 것이 대표적으로 밝혀진 기전이다 11. 질병관리본부에 따르면, 미세먼지(PM 10) 농도가 10 μg/m 3 증가할 때마다 만성폐쇄성폐질환(COPD)으로 인한 입원율은 2.7%, 사망률은 1.1% 증가한다고 보고되었으며, 미세먼지(PM 2.5) 농도가 10 μg/m 3 증가할 때마다 폐암 발생률이 9% 증가하는 것으로 나타나 12 호흡기질환자는 미세먼지에 장기간 노출되지 않도록 권고하고 있다. 미세먼지로 인한 사회⋅경제적 손실이 증가하고 미세먼지로부터 인체 호흡기계 질환을 예방하기 위한 대책이 시급한 시점에서, 본 연구에서는 미세먼지의 호흡기 관련 임상연구 동향을 조사하여 연구 방법 및 특성에 대해 알아보고 향후 이를 위한 임상연구 방법을 모색하는데 도움이 되고자 하였다. 또한, 지금까지 미세먼지를 포함하는 다양한 대기오염의 호흡기 관련 연구들이 많이 진행되어왔으나, 본 연구에서는 미세먼지의 호흡기영향 관련 연구에 초점을 맞추고자 미세먼지로 국한하여 관련 문헌들을 조사하고 분석하였다.
II. 연구대상 및 방법
1. 연구 대상
본 연구에서는 미세먼지 관련 호흡기질환 임상연구 동향을 조사하기 위하여 PubMed, EMBASE, the Cochrane Central Register of Controlled Trials (CENTRAL)의 3가지 해외 데이터베이스를 검색원으로 사용하였으며, 2019년 05월까지 발표된 관찰연구와 중재연구를 포함하는 모든 임상연구를 대상으로 조사하였다. 언어는 영어로 제한을 두었으며, 미세먼지와 관련된 용어가 다양하여 particulate matter의 MeSH Term으로 Pubmed에서 제시된 Entry Term만을 사용하여 다음의 검색식으로 검색하였다(Particulate Matter[Title] OR Airborne Particulate Matter[Title] OR Particulate Matter, Airborne[Title] OR Air Pollutants, Particulate [Title] OR Particulate Air Pollutants[Title] OR Pollutants, Particulate Air[Title] OR Ambient Particulate Matter[Title] OR Particulate Matter, Ambient[Title]) Filters: Clinical Trial; Humans. [검색 일시] : 2019년 05월 08일
검색 결과 총 150편의 논문이 검색되었으며 1차적으로 제목 및 초록을 검토하여 중복되는 논문, 호흡기질환과 관련되지 않은 논문을 배제하여 24편의 논문을 선별하였다. 원문을 바탕으로 2차 screening을 시행하여 원문을 찾을 수 없는 경우(n=1), 임상연구가 아닌 경우(n=1), 영어가 아닌 경우(n=1), 미세먼지가 major topic이 아닌 경우(n=3)를 제외하여 최종적으로 18편의 논문 13-30을 연구대상으로 선정하였다( Fig. 1).
Fig. 1
Flowchart of study selection process. 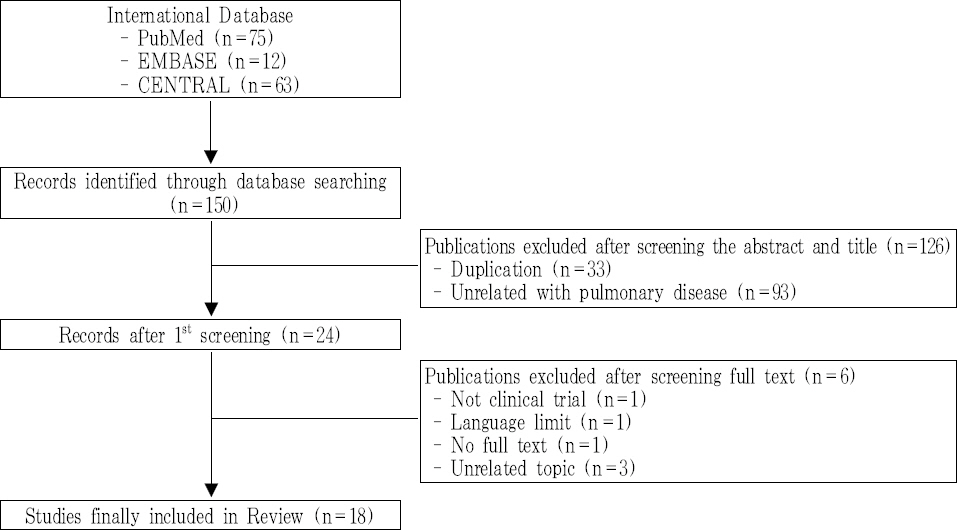
2. 연구 방법
두 명의 연구자(LYU, KIM)가 독립적으로 제목 및 초록과 원문을 바탕으로 선정 기준에 맞지 않은 문헌을 배제하였으며, 의견이 불일치하거나 합의가 이루어지지 못할 경우 제 3의 연구자(PARK)에게 자문을 구하여 최종 포함여부를 결정하였다.
본 연구에서는 최종 선정된 총 18편 문헌들의 연구개요 및 특성, 연구 종류 및 디자인, 대상 질환, 대상자 수 및 특성, 연구 및 중재 기간, 평가 변수, 연구 결과, 미세먼지 관련 측정 범위 및 방법에 대하여 분석하고 고찰하였다.
III. 결 과
1. 연구개요 및 특성
미세먼지는 실내⋅외에서 모두 발생하여 인체 내 유해영향을 미치며, 본 연구에서 최종 선별된 18편의 논문 중 실외 미세먼지의 호흡기 영향에 관한 연구가 15편, 실내 미세먼지의 영향을 보고자 한 연구가 3편에 해당되었다.
미세먼지 관련 호흡기질환 임상연구의 연도별 분포는 1985년을 시작으로 2018년까지 점차 증가하는 추세를 보였으며, 1980년대 1편, 1990년대 1편, 2000년대 5편, 2010년 이후 현재까지 11편의 관련 논문들이 발표되었다( Fig. 2). 기존의 대기오염 연구에서는 총 먼지(TSP), 먼지 등의 다양한 지표로 평가가 이루어졌으나, 1980년대 중반 이후부터 상대적으로 작은 크기의 입자상 물질인 미세먼지(PM)에 초점이 맞춰지게 되면서 미세먼지 관련 연구가 1980년대 중반 이후 점차 증가해온 것을 볼 수 있다.
Fig. 2
Number of articles in chronological sequence. 
해당 연구들이 시행된 지역은 대부분 북미와 유럽 그리고 일부 아시아 국가들이었으며, 미국 및 캐나다가 10편으로 가장 많은 수를 차지하였다. 그 외, 중국 3편, 일본 1편, 덴마크 1편, 과테말라 1편의 지역 분포를 보였으며, 유럽의 여러 국가 및 전 세계 55개 국가들을 대상으로 한 연구가 각각 1편씩 존재하였다( Table 1).
Table 1
Characteristics of the Studies Included in the Review
|
First author |
Article title |
Year |
Region |
Study design |
Subject condition |
# of subjects |
Ages (years) |
Air pollution monitoring |
|
1 |
Kleinman, M. T.13
|
Controlled exposure to a mixture of SO2, NO2, and particulate air pollutants: effects of human pulmonary function and respiratory symptoms. |
1985 |
USA |
RCT (cross-over) |
Healthy |
20 |
18-55 |
ZnSO4, (NH4) 2SO4, NO2, SO2
|
|
|
2 |
Wang, B14
|
Particulate matter, sulfur dioxide, and pulmonary function in never-smoking adults in Chongqing, China. |
1999 |
China |
Cross-sectional study |
Healthy |
1,075 |
35-60 |
PM2.5, SO2
|
|
|
3 |
Gong, H.15
|
Controlled exposures of healthy and asthmatic volunteers to concentrated ambient fine particles in Los Angeles. |
2003 |
USA |
RCT (cross-over) double-blind |
Asthma |
24 |
18-45 |
CAP |
|
|
4 |
Slaughter, J. C.16
|
Effects of ambient air pollution on symptom severity and medication use in children with asthma. |
2003 |
USA |
Retrospective cohort study |
Asthma |
133 |
5~12 |
PM2.5, PM10, CO |
|
|
5 |
Schildcrout, J. S.17
|
Ambient air pollution and asthma exacerbations in children: an eight-city analysis. |
2006 |
USA, Canada |
Retrospective cohort study |
Asthma |
990 |
5~12 |
CO, NO2, SO2, O3, PM10
|
|
|
6 |
Bedada, G. B.18
|
Urban background particulate matter and allergic sensitization in adults of ECRHS II. |
2007 |
Europe |
Cross-sectional study |
Healthy |
6,470 |
20-44 |
PM2.5, SO2
|
|
|
7 |
Qian, Z.19
|
Interaction of ambient air pollution with asthma medication on exhaled nitric oxide among asthmatics. |
2009 |
USA |
Retrospective cohort study |
Asthma |
119 |
12-65 |
NO2, PM10, O3, SO2
|
|
|
8 |
Anderson, H. R.20
|
Ambient particulate pollution and the world-wide prevalence of asthma, rhinoconjunctivitis and eczema in children: Phase One of the International Study of Asthma and Allergies in Childhood (ISAAC). |
2010 |
51 countries |
Cross-sectional study |
Healthy |
513,153 |
6-7, 13-14 |
PM10
|
|
|
9 |
Roy, A.21)
|
Ambient particulate matter and lung function growth in Chinese children. |
2012 |
China |
Prospective cohort study |
Healthy |
3,273 |
6-12 |
PM2.5, PM10
|
|
|
10 |
Karottki, D. G.22
|
An indoor air filtration study in homes of elderly: cardiovascular and respiratory effects of exposure to particulate matter. |
2013 |
Denmark |
RCT (cross-over) double-blind |
Healthy |
49 |
>51 |
CAP |
|
|
11 |
Alexis, N. E.23
|
Patients with asthma demonstrate airway inflammation after exposure to concentrated ambient particulate matter. |
2014 |
USA |
RCT (cross-over) single blind |
Asthma |
10 |
18-45 |
PM |
|
|
12 |
Guarnieri, M.24)
|
Lung function in rural guatemalan women before and after a chimney stove intervention to reduce wood smoke exposure results from the randomized exposure study of pollution indoors and respiratory effects and chronic respiratory effects of early childhood exposure to respirable particulate matter study. |
2015 |
Guatemala |
Prospective cohort study |
Healthy |
265 |
39-84 |
CO |
|
|
13 |
Kariisa, M.25
|
Short- and long-term effects of ambient ozone and fine particulate matter on the respiratory health of chronic obstructive pulmonary disease subjects. |
2015 |
USA |
Retrospective cohort study |
COPD |
1,218 |
39-84 |
PM2.5, O3
|
|
|
14 |
Zhou, Y.26
|
Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease: results from a cross-sectional study in China. |
2016 |
China |
Cross-sectional study |
COPD |
5,993 |
≥20 |
PM2.5, PM10
|
|
|
15 |
Meliton, A. Y.27
|
Short-term acute exposure of healthy humans to particulate matter induces differential gene expression in lung immune cells. |
2017 |
USA |
RCT |
Healthy |
6 |
18-40 |
PM2.5
|
|
|
16 |
Watanabe, M.28
|
A panel study of airborne particulate matter composition versus concentration: Potential for inflammatory response and impaired pulmonary function in children. |
2017 |
Japan |
Prospective cohort study |
Healthy |
339 |
10~12 |
SPM, PM2.5, SO2, NO2, O3
|
|
|
17 |
Holm, S. M.29
|
Cooking behaviors are related to household particulate matter exposure in children with asthma in the urban East Bay Area of Northern California. |
2018 |
USA |
Prospective cohort study |
Asthma |
35 |
6~10 |
PM2.5
|
|
|
18 |
Pirozzi, C. S.30
|
Short-Term Particulate Air Pollution Exposure is Associated with Increased Severity of Respiratory and Quality of Life Symptoms in Patients with Fibrotic Sarcoidosis. |
2018 |
USA |
Retrospective cohort study |
Fibrotic Sarcoidosis |
16 |
18-70 |
PM2.5, O3
|
2. 연구 종류 및 디자인
최종 선별된 18편의 논문은 크게 관찰연구와 시험연구로 분류될 수 있으며 관찰연구가 13편, 시험연구가 5편에 해당된다. 대다수를 차지하고 있는 13편의 관찰연구 중 단면연구는 4편, 코호트 연구는 9편에 해당되며, 코호트 연구의 경우 전향적 코호트 연구가 4편, 후향적 코호트 연구가 5편에 해당된다( Fig. 3).
Fig. 3
Study design of selected studies. 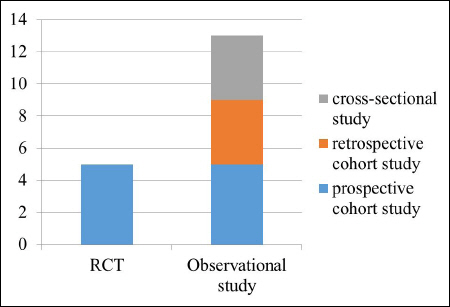
중재가 있는 시험연구 5편은 모두 무작위대조 임상실험(Randomized controlled trial, RCT)으로 미세먼지 혹은 대조물질을 대상자에게 노출시켜 각 군의 차이를 보고자 하였다. 시험 설계는 이중 맹검으로 시행된 경우가 3편, 단일 맹검으로 시행된 경우가 1편, 명시되지 않은 경우가 1편 있었으며, 그 중 4편에서는 cross-over 디자인으로 설계되었다( Table 1).
3. 연구 대상 질환
본 연구에서 조사된 호흡기 관련 대상 질환은 천식 7편, 만성폐쇄성폐질환(COPD) 2편, 섬유성 사르코이드증 1편으로 천식 관련 연구가 가장 많았으며, 그 외의 논문에서는 건강인을 대상으로 하여 호흡기관련 폐기능, 호흡기 부작용, 알레르기 반응, 유전자발현에의 영향 등을 보고자 하였다( Table 1).
4. 연구 대상자 수 및 특성
연구 대상자 수는 관찰연구의 경우 최소 16명에서부터 최대 513,153명까지 다양하였으나 1,000명이상의 대규모로 진행된 연구가 많았으며, 시험연구에서의 대상자 수는 평균 21.8명으로 최소 6명에서 최대 49명까지의 분포를 보여 비교적 대상자 수는 적은 편이나 대부분 cross-over로 설계되어 이를 보완하였다.
대상자의 연령은 소아와 성인 등으로 다양하였으며, 소아를 대상으로 한 경우가 6편, 성인을 대상으로 하는 경우가 10편, 소아와 성인 모두를 대상으로 하는 경우가 2편에 해당되었다. 구체적으로 소아의 경우 5~12세, 6~10세, 10~12세, 12~13세 등의 여러 연령을 대상으로 연구가 진행되었으며, 성인의 경우도 18~45세, 18~70세, 35~60세, 51세 이상 등으로 대상자의 연령대가 연구 대상 질환 및 목적에 따라 다양하게 설계되었다. 천식의 경우 고령자는 포함시키지 않고 45세 이하로 한정시키는 연구가 많았으며, 만성폐쇄성폐질환(COPD)의 경우 39~84세까지로 대상자의 연령 범위를 넓게 설정하거나 나이의 상한을 두지 않는 등으로 고령자를 포함시켜 질환의 역학 및 특성을 고려하기도 하였다. 기타 연구 목적에 따라 노인들의 심폐기능의 변화를 보고자 하는 연구에서는 51세 이상의 대상자만 포함시키는 경우 및 폭넓게 소아와 성인 모두를 대상자로 포함시키기는 연구도 있었다( Table 1). 기타 미세먼지 관련 임상연구에서는 대상자 모집 시 특징적으로 대상자의 거주지가 미세먼지 측정 장소 혹은 대로로부터 가까운 곳에 위치한 자로 제한을 두거나 흡연자 혹은 실내에서 석탄을 사용하는 경우는 연구에서 배제시키는 경우를 볼 수 있다. 관찰연구 5편에서 대상자의 거주지가 미세먼지 측정 장소로부터 1~2 km 혹은 80 km이내인 자로 제한을 두었으며, 실내 미세먼지의 영향을 보기 위한 1편의 시험연구에서는 외부 미세먼지의 농도 영향을 균일하게 하기 위한 노력으로 대상자의 거주지가 대로로부터의 35 m 이내인 자로 제한하여 모집을 진행하였다 22. 또한 실내에서 석탄을 사용하는 경우를 제한하는 연구 14 및 흡연자를 연구대상자에서 제외된 경우 14,19,23,27는 4편의 논문에서 볼 수 있었다.
5. 연구 및 중재 기간
관찰연구 중 단면연구를 제외한 9편의 코호트 연구에서의 연구기간은 평균 26.8개월로 최소 1개월에서부터 최대 10년까지의 분포를 보였으며, 연구기간이 2년인 경우가 가장 많았다. 연구기간이 1개월인 연구 2편은 모두 전향적 코호트 연구로 미세먼지의 단기 영향을 보고자 하였으며, 나머지 7편의 연구에서는 모두 최소 2년 이상을 관찰하여 결과를 도출하였다( Table 2).
Table 2
Summary of Observational Studies
|
First author |
Observation period |
Subject data source |
Inclusion/exclusion criteria |
Outcome measures |
PM update |
Results |
|
Wang, B |
1995.01 -1995.12 |
survey |
1) adults 35 to 60 years of age who had never smoked and did not use coal stoves for cooking or heating
2) restricted to administrative staff members and officials at the study sites within 1km of the air monitoring site |
1) lung function (FEV1, FVC, FEV1/FVC%) |
daily |
Significant difference of FEV1 between the urban and suburban areas. |
|
|
Slaughter, J. C. |
1993.11 -1995.09 |
Seattle CAMP |
1) children from 5 through 12 years of age
2) mild-to-moderate asthma, as defined by the presence of symptoms or by the use of an inhaled bronchodilator at least twice weekly or the use of daily medication for asthma
3) excluded if the concentration of methacholine causing a 20% decrement in forced expiratory volume in 1 second (FEV1PC20), was greater than 12.5 mg/mL and any other clinically significant conditions. |
1) inhaler use
2) asthma severity |
daily |
PM2.5, PM10, and CO concentrations significantly associated with asthma severity and medication use in a population of children with mild-to-moderate asthma severity. |
|
|
Schildcrout, J. S. |
1993.11 -1995.09 |
CAMP |
1) children from 5 through 12 years of age
2) mild-to-moderate asthma, as defined by the presence of symptoms or by the use of an inhaled bronchodilator at least twice weekly or the use of daily medication for asthma
3) excluded if the concentration of methacholine causing a 20% decrement in forced expiratory volume in 1 second (FEV1PC20), was greater than 12.5 mg/mL and any other clinically significant conditions.
4) excluded if we were able to verify that the centroid of the ZIP or postal code in which they lived was greater than 50 miles (80 km) from the nearest Aerometric Information Retrieval System pollutant monitor |
1) inhaler use
2) asthma severity
3) sum of the two within-subject pollutant effects |
daily |
CO, NO2 were significantly associated with asthma severity and medication use in a population of children with mild-to-moderate asthma severity. |
|
|
Bedada, G. B. |
1990-2000 |
survey |
1) aged 20-44 years
2) responded to the main questionnaire
3) presence of air pollution measurement in the particular centre
4) presence of IgE measurement |
1) allergic sensitization (IgE) |
annually |
Regional air pollution is not associated with allergic sensitization among adults in ECRHS II. |
|
|
Qian, Z. |
1997.02 -1999.01 |
SOCS |
1) aged 12-65 years
2) nonsmokers
3) asthmatics
4) presence of samplings of eNO |
1) eNO Measurements |
daily |
NO2 and PM10 were significantly associated with an increase in exhaled nitric oxide (eNO) and medication could not counteract airway inflammation effects of air pollution. |
|
|
Anderson, H. R. |
1999 |
ISAAC |
1) 6-7, 13-14 year old children from a self-completed questionnaire at school |
1) prevalence of asthma, rhinoconjunctivitis, eczema |
annually |
PM10 has no association with the prevalence of childhood asthma, rhinoconjunctivitis or eczema. |
|
|
Roy, A. |
1993-1996 |
survey |
1) children 6–12 years in 8 districts within the 4 cities
2) their families had no plans to move within 3 years
3) their homes were within 2 km of the schools |
1) lung function (FEV1, FVC) |
daily |
PM2.5 and PM10 significantly associated with lung function growth. |
|
|
Guarnieri, M. |
2008.12 -2009.03 |
RESPIRE + survey |
1) aged 15-50 years
2) all using traditional indoor open fires |
1) lung function (FEV1, FVC)
2) wood Smoke Exposure Assessment : EB co, personal CO tube measurements |
- |
No association between lung function and early randomization to a chimney stove or personal wood smoke exposure |
|
|
Kariisa, M. |
1998-2002 |
NETT |
1) aged 39-84
2) sever bilateral emphysema |
1) lung Function (FEV1, FVC)
2) respiratory Outcomes : Respiratory morbidity, St. George’s Respiratory Questionnaire |
daily |
Significant association between air pollution and respiratory function and symptoms of severe COPD subjects |
|
|
Zhou, Y. |
2012-2015 |
survey |
1) aged≥20 years
2) COPD (defined as a post-bronchodilator FEV1/FVC less than 70%) |
1) lung function (FEV1, FVC)
2) Questionnaire and risk factors for COPD : revised from the international BOLD (Burden of Obstructive Lung Diseases) study, including possible risk factors for COPD |
annually |
PM concentration was strongly associated with increased COPD prevalence and declined respiratory function. |
|
|
Watanabe, M. |
2015.02.01 -2015.02.28 |
survey |
1) students aged 10-12 years in four elementary schools in Matsue City
2) all subjects lived within a 1-km radius from the schools which these four elementary schools were within 10 km of each other |
1) morning peak expiratory flow (PEF)
2) THP1 cells 3) IL-8 |
daily |
IL-8 levels were significantly associated with SPM and PM2.5 and no significant relationships between PEF, SPM, and PM2.5. |
|
|
Holm, S. M. |
2015.11 2016.11 2016.04 |
survey |
1) children aged 6-10
2) physician-diagnosed asthma but no other major illnesses
3) excluded if they had severe asthma exacerbation requiring systemic steroids in the last 3 months, not compliant with asthma medications, using albuterol daily and not on maximal controller therapy, a smoker in the home was a minor, another participant’s sibling or their parent or adult smoker was functionally illiterate in written English |
1) Asthma severity
2) household factors : hood fan use, presence of a cigarette smoker, distance from the highway, presence of pets, heater use and outdoor PM2.5 levels |
monthly |
The relationship between mean PM2.5 and asthma severity approached significance for persistent versus intermittent asthma for every 5 μg/m3 increase in the monthly mean PM2.5 level. |
|
|
Pirozzi, C. S. |
2013.06 -2015.06 |
Double Blind, Placebo Controlled Study of Roflumilast to Prevent Acute Events in Fibrotic Sarcoidosis |
1) between 18 and 70 years of age
2) a diagnosis of sarcoidosis by American Thoracic Society (ATS) criteria
3) exclusion criteria included renal dysfunction with creatinine >3 mg/dL, moderate or severe liver disease, unstable cardiac disease, non-cutaneous malignancy treated in the past two years, unable to complete questionnaires or lung function testing |
1) lung function (FEV1, FVC, episodes of FEV1 decline greater than 10% from each individual’s highest value)
2) questionnaires: LCQ, SGRQ, KSQ |
daily |
PM2.5 levels were not associated with FEV1, FVC, episodes of FEV1 decline >10%, or respiratory symptoms measured by SGRQ or LCQ, but associated with severity of respiratory and quality of life symptoms using KSQ. Ozone exposure was not associated with any health outcomes. |
시험연구 5편 중 4편의 논문은 실외 미세먼지의 영향을, 1편의 논문은 실내 미세먼지의 영향을 보고자 하였으며 이에 따라 중재 기간이 다르게 설정되었다. 실외 미세먼지의 영향을 보고자하는 4편의 연구에서 중재 기간은 2시간 혹은 2시간 15분이었으며, 그 중 cross-over 디자인으로 설계된 3편의 연구에서 wash out 기간은 2~4주로 설정되었다. 실내 미세먼지의 영향을 보는 1편의 연구의 중재 기간은 14일로 설정되었으며 cross over 디자인으로 설계되었다( Table 3).
Table 3
Summary of Randomized Controlled Trials
|
First author |
Intervention |
duration |
Inclusion/exclusion criteria |
Outcome measures (time frame) |
Results |
|
Kleinman, M. T. |
1) control : NaCl
2) test : NaCl + ZnSO4, (NH4) 2SO4, NO2, SO2 |
2 h 15 min (wash-out 3-4 weeks) |
1) aged between 18-55
2) absense of any medical contraindications as determined by lung function test and an abbreviated cardiac stress test |
1) pulmonary function (pre, post) : FVC, FEV1, FEV2, PEFR, FEF50%, FEF75%, TLC, RV, CV/VC%, CC/TLC%, delta N2, total resistance of the respiratory tract (R)
2) exposure relatable symptoms (pre, post, 1, 7 day) |
not significant |
|
|
Gong, H. |
1) control : FA (filtered air)
2) test : CAP (concentrated ambient air) |
2h (wash-out 14 days) |
1) aged 18-45
2) healthy and asthmatic nonsmoking volunteers screened by history and physical examination, lung function tests, submaximal exercise stress test, and pregnancy test for females
3) asthmatics tested for atopy and nonspecific bronchial hyper-reactivity |
1) symptom questionnaire (pre, post, 4 hours, 2 days)
2) blood pressure (pre, post, 4 hours, 2 days)
3) heart rate (pre, post, 4 hours, 2 days)
4) SaO2 (pre, post, 4 hours, 2 days)
5) lung function (FEV1, FVC) (pre, post, 4 hours, 2 days)
6) venous blood sampling (IL-6 and IL-8, serum amyloid A, ICAM-1, fibrinogen, factor VII, and von Willebrand factor, fibrinogen, factor VII, and von Willebrand factor) (pre, post, 4 hours, 2 days)
7) sputum (IL-6, IL-8, ECP) (2 days)
8) Holter ECG (entire first and second intervals, ventricular and supraventricular arrhythmia incidence, measures of heart rate variability) (pre-4 hours, 4 hours-2 days) |
not significant |
|
|
Karottki, D. G. |
1) control : sham air filtration
2) test : active air filtration |
14 days |
1) aged over 51 years and living in Greater Copenhagen in non-smoking apartments within 350 m (min 25 m, max 1000 m) from major roads (>10,000 vehicles per day) |
1) blood pressure (day 0, 2, 7, 14)
2) peripheral arterial tonometry (day 0, 2, 7, 14)
3) lung function (FEV1, FVC) (day 0, 2, 7, 14)
4) biomarkers in blood (C-reactive protein (CRP), hemoglobin, leukocytes, lymphocytes, monocytes, granulocytes, CD31, CD62L, CD11b, CD49d, CC16, SPD) (day 0, 2, 7, 14) |
not significant |
|
|
Alexis, N. E. |
1) control : FA (filtered air)
2) test : CAP (concentrated ambient air) |
2h (wash-out 4 weeks) |
1) asthmatics aged 18-45
2) nonsmokers with mild to moderate disease severity |
1) BW, BAL : PMNs, IL-1b, IL-8, IL-6, TNF-a, CD40 ligand (CD40L), E-selectin, soluble vascular cell adhesion molecule-1 (sVCAM1), plasminogen, fibrin, C-reactive protein (CRP), fibrinogen, soluble intercellular adhesion molecule-1 (sICAM-1), myeloperoxidase (MPO), CD11b/CR3, CD64/FcgRI, CD40, CD86/B7.2, CD16/FcgRIII, low-affinity IgE receptor (CD23) (20 hours)
2) lung function (FEV1, FVC) (pre, 20 hours) |
significant |
|
|
Meliton, A. Y. |
1) control : FA (filtered air)
2) test : PM (diesel exhaust particles) |
2 h |
1) non-smoker subjects
2) between the ages of 18 and 40
3) no history lung disease or active medical problems |
1) RNA sequencing (differential expressed genes (DEGs)) (24 hours) |
significant |
6. 평가 변수
본 연구는 다양한 호흡기관련 질환을 포함하고 있어 해당 질환 및 연구 목적에 따라 보고자 하는 평가변수 또한 다양하게 설정되었다. 호흡기와 관련하여 가장 많이 사용된 평가변수는 폐 기능이었으며 총 9편의 논문에서 폐기능검사(spirometer)를 하여 1초간 노력성 호기량(FEV1, forced expiratory volume in one second) 및 노력성 폐활량(FVC, forced vital capacity)을 측정하였다. 호흡기 관련 증상 설문을 시행한 경우는 7편에 해당하였으며 그 중 호흡기관련 삶의 질 평가척도인 St. George’s Respiratory Questionnaire(SGRQ)을 사용한 경우가 3편에서 있었고 그 외 Leicester cough questionnaire(LCQ)와 King’s Sarcoidosis Questionnaire(KSQ)가 1편의 연구에서 사용되었다. 혈액검사를 시행하여 염증 반응 혹은 응고 관련 인자를 보고자 하는 경우는 5편에서 나타났으며, IL-8을 보는 경우가 3편에 해당하였고 그 외 IL-6, serum amyloid A, ICAM-1, fibrinogen, factor VII, von Willebrand factor, fibrinogen, IgE를 측정하였다. 기관지폐포세척(BAL, bronchoalveolar lavage fluid)과 기관지세척(BW, bronchial wash)에서 PMNs, IL-1b, IL-6, IL-8, TNF-a을 측정한 경우와 객담에서 WBC, neutrophil, IL-6, IL-8를 측정하는 경우도 각각 1편의 논문에서 볼 수 있었다. 기타 질환 특이적인 척도로 천식환자들의 경우 천식 중증도 평가를 시행한 경우가 3편에서 나타났으며, 연구 목적에 따라 혈압, 말초동맥 긴장도, Holter ECG, 6분 보행검사, SaO2, PEFR, eNO, RNA sequencing이 측정되었다( Table 2, 3).
7. 연구 결과
미세먼지가 인체 호흡기에 미치는 영향을 연구한 총 18편의 논문 중 통계적으로 유의미한 결과는 관찰연구에서 9편, 시험연구에서 2편에서 보고되었으며, 그 외의 연구에서는 호흡기와의 연관성만 제시되었다. 다만, 단기 노출 평가를 진행한 5편의 무작위배정 연구에서는 2편에서만 유의미한 결과가 도출되어 미세먼지의 단기 노출이 호흡기에 미치는 영향은 일관된 결과를 보이지 않는 것으로 볼 수 있다( Table 2, 3).
8. 미세먼지 관련 자료
1) 미세먼지 범위
각 연구에서는 미세먼지를 포함한 다양한 대기오염물질을 측정하여 호흡기 질환과의 관련성을 보고자 하였으며 연구마다 측정하는 대기오염물질의 종류와 크기는 다양하였다. 13편의 관찰연구 중 1편의 실내 미세먼지 관련 연구를 제외한 12편의 논문에서 PM 농도 측정값을 사용하였으며, 그 중 PM2.5만을 측정한 경우가 6편, PM10만을 측정한 경우가 3편, PM2.5와 PM10 모두를 측정한 경우가 3편에 해당되었다. 미세먼지와 함께 측정된 대기오염물질로는 SO2, NO2, O3, CO가 있었으며 SO2는 5편, O3 5편, NO2 3편, CO 3편에서 측정되었다.
5편의 시험연구에서 대상자에게 노출되는 중재물질로 사용된 미세먼지의 구성과 농도는 연구마다 상이하였다. 실외 미세먼지 연구에서는 중재물질로 CAP(concentrated ambient air)가 2편, PM (particulate matter)이 1편, 기타 복합물(NaCl + ZnSO 4, (NH 4) 2SO 4, NO 2, SO 2)이 1편에서 사용되었고, 대조물질로는 FA(filtered air)가 3편, NaCl이 1편에서 사용되었다. 중재물질로 사용된 CAP 혹은 PM은 용어의 차이는 있으나 모두 PM 농도 101.8~250 μg/cm 3의 분포를 보이는 대기오염물질로 실제 외부 미세먼지와 동일하게 구성하고자 하였다. 실내 미세먼지 연구에서는 sham air filtration, active air filtration을 사용하여 양측 실내 미세먼지 농도에 차이를 두어 농도 별 평가변수를 측정하여 비교하였다( Table 1).
2) 미세먼지 측정방법
관찰연구에서 미세먼지 측정은 직접 측정하거나 각 국가 또는 지역에서 제공하는 기상 자료를 사용하였다. 분석 시 미세먼지 농도는 일일, 월별 혹은 연간 평균값을 사용하였으며 측정값의 오차를 줄이기 위하여 동일 시각에 측정하거나 측정 장비의 질 평가를 지속적으로 시행하였다( Table 2). 시험연구 중 실내 미세먼지 관련 연구에서는 침실과 거실 2곳에서 2주 동안 미세먼지 농도를 측정하였고 그 외 4편의 연구에서는 대상자의 노출이 이루어지는 좁은 방안의 농도를 노출시간 동안 측정하였다.
IV. 고 찰
세계보건기구(WHO)는 미세먼지 노출에 의한 장⋅단기 건강영향평가에서 미세먼지가 단기적으로는 폐의 염증반응 및 호흡기증상의 악화를 일으키고, 장기적으로는 COPD의 급성악화 및 사망률의 증가와 폐암 발생위험도 증가, 하기도 증상 증가, 폐기능 저하, 폐기능 감소 속도 증가에 영향을 미치는 것으로 보고하였다 4. 미세먼지는 체내에 침착되고 일부는 혈액을 따라서 전신을 순환하면서 산화 스트레스와 염증 반응을 일으키게 되며 31,32, 산화스트레스, 기도개형, 선천면역 및 후천면역 등의 기전에 의해 인체에 영향을 미친다 33. 전 세계적으로 1980년대 중반 이후 입자의 크기가 작을수록 인체의 건강에 미치는 영향이 크다는 결과들이 발표되면서 34 미세먼지가 중요한 대기오염 물질로 인식되기 시작하였으며, 우리나라에서도 국립환경과학원을 중심으로 2000년도부터 미세먼지에 대한 특성 분석 및 건강 관련 다양한 연구들이 이루어졌다 35. 이에 본 연구에서도 다양한 대기오염 물질 중 미세먼지에 초점을 맞추어 미세먼지로 국한하여 문헌조사를 시행하였다. 본 연구에서 최종 선별된 18편의 논문들 또한 1985년부터 2018년까지 점차 증가하는 추세를 보였으며, 위 연구들은 북미, 유럽 및 일부 아시아 국가들에서 발표되었다. 국내에서도 미세먼지의 천식 36 및 폐암 12, 호흡기질환자 입원 일수 37 등에 미치는 영향에 대한 연구가 진행되어 왔으나, 장기 노출 영향 평가 및 다양한 호흡기 질환에의 연구 결과는 아직 부족한 실정이다 38. 최종 선별된 18편의 논문들을 고찰한 결과, 지금까지의 미세먼지 관련 임상연구들은 대부분 관찰연구로 진행되었으며 장⋅단기의 미세먼지 노출 영향을 보기 위해 코호트 연구 형태로 설계된 경우가 가장 많은 것을 관찰 할 수 있었다. 무작위배정 임상시험(RCT)의 경우 인체에 유해하다고 판단되는 미세먼지를 대상자에게 직접 노출시키는 것에 대한 윤리적인 문제 및 장기 노출 평가가 어렵다는 측면에서 거의 이루어지지 않았으며, 본 연구에서 조사한 5편의 무작위배정 임상시험 논문들에서 또한 위의 한계점을 보완하기 위하여 노출시키는 중재물질을 비교적 안전한 질산염 및 황산염 등의 복합물로 재구성하거나 농도를 실제 대기 중의 미세먼지 농도와 비슷한 수준으로 설정하는 등의 노력을 기울였다. 향후 미세먼지의 건강 영향 관련 임상 연구들 또한 무작위배정 임상시험으로 진행되기에는 연구의 한계 및 윤리적인 문제점이 있을 것으로 생각되며 39 그 외의 연구 형태로 임상연구가 진행되어야 할 것이다. 지금까지 가장 많이 시행된 코호트 연구의 경우 처음부터 연구 목적으로 연구 대상자들을 모집하여 자료를 수집하는 ‘전향적 코호트 연구’ 또는 기존 자료를 기반으로 이미 수집된 자료를 이용하여 분석하는 ‘후향적 코호트 연구’ 형태로 연구의 목적에 따라 설계되어 진행되어 왔다. 전향적 코호트 연구는 결과에 의해 예측 변수 측정값이 영향 받는 것을 방지하므로 변수들을 보다 정확하게 측정할 수 있다는 장점이 있으나 시간과 비용이 많이 들고 빈도가 낮은 결과를 분석할 때에는 효율이 떨어진다는 단점이 있다 40. 반면, 후향적 코호트 연구는 예측변수의 특성 및 품질에 관해 연구자의 역할이 제한되어 있어, 보다 정확한 예측 변수의 측정을 위해 전향적 연구 형태로 설계된 다양한 연구가 진행될 필요가 있으며, 장기간의 관찰 기간을 기반으로 한 후향적 코호트 연구 또한 진행되어야 할 것으로 생각된다. 따라서, 향후 한약제제의 항 미세먼지 효과에 대한 임상연구 설계 시에도 무작위배정 임상시험으로 설계하는 것은 여러 한계 및 제한이 있으므로, 대상자의 거주지 혹은 작업환경 등에서의 미세먼지 노출 정도를 고려한 코호트 등의 관찰 연구 형태를 고려해 볼 수 있을 것이다. 또한, 최근 실내 미세먼지의 유해성에 대한 관심이 늘어나고 있는 시점에서 41, 한방진료에서 사용되고 있는 뜸 치료 등과 관련하여 한방의료기관 내의 실내미세먼지 영향에 대한 연구 등이 고안될 수 있을 것이다. 미세먼지의 호흡기 영향에 대한 연구들은 천식 16,17,19,23,29,42 관련 연구가 가장 많이 보고되었으며 COPD 25,26, 간질성폐질환 30 및 건강인의 폐기능 혹은 호흡기 증상 관련 연구 13,14,18,20-22,24,27,28들이 진행되어 왔다. 대상자의 질환 및 연령은 연구 목적에 따라 다양하게 설정될 수 있으며 미세먼지 관련 연구에서는 대상자 모집 시 대상자 및 동반 거주자의 흡연력, 거주지와 대로와의 거리, 반려동물 유무 및 실내 환경 등을 동시에 조사하여 혼란 변수(confounding factor)에 대한 고려가 반드시 필요하다. 호흡기 영향을 평가하기 위한 평가도구로는 폐기능검사 13-15,21-26,30가 대표적이며 호흡기 증상 관련 설문지 15,25,26,30, 혈액 및 객담에서의 biomarker 15,18,19,22-24,28 등이 측정될 수 있다. 호흡기 질환의 삶의 질 평가도구로는 신뢰도 및 타당도가 입증 된 St. George’s Respiratory Questionnaire(SGRQ) 25,30가 활용될 수 있으며, 혈액 및 객담에서의 biomarker로 WBC, neutrophil, CRP, fibrinigen, IgE, IL-6, IL-8, TNF-a 등 15,22,23,28이 호흡기 영향을 보기 위한 평가변수로 사용될 수 있다. 본 연구에서 선별된 18편의 논문 중 총 11편에서 미세먼지의 호흡기 영향에 대한 평가가 통계적으로 유의미한 결과가 있는 것으로 발표되었다. 그 외, 유의미한 결과를 도출하지 못한 연구들에서는 대기 노출 평가의 방법이 엄격하지 못한 점, 연구의 관찰기간이 짧은 점, 혼란 변수의 영향을 배제하지 못한 점 등을 연구의 한계점으로 제시하고 있다. 따라서 향후에는 장기간의 관찰기간과 대상자의 대기 노출 평가와 혼란 변수를 조절하기 위한 노력 등이 요구되며, 이를 위해서는 미세먼지 측정 시 PM2.5와 PM10으로 PM의 크기에 따라 분류하여 미세먼지의 측정이 이루어져야 하고, 미세먼지 측정 시간 및 주기가 일정하게 이루어지고 미세먼지 측정 장비의 정도 관리가 주기적으로 이루어질 수 있도록 미세먼지 측정에 대한 규정이 만들어져야 할 것이다. 또한, 미세먼지 측정 장소와 연구 대상자의 미세먼지 노출 상관관계를 높이기 위하여 대상자의 거주 위치, 흡연 유무, 작업 환경, 외부공기 노출 시간 등의 혼란 변수에 대한 고려도 반드시 이루어져야 한다.
국내외 다양한 미세먼지의 호흡기관련 임상연구들이 진행되어왔으나 미세먼지의 약물치료에 대한 연구는 아직까지 보고된 바가 거의 없다. 2015년 대한 결핵 및 호흡기학회에서 발간된 ‘미세먼지/황사 건강피해 예방 및 권고지침‘에서도 약물치료에 대한 권고사항은 제시되지 않았으며, 호흡기 환자들에게 외출 시 방역용 마스크를 사용할 것과 미세먼지 예보 등급을 참고하여 외출을 자제 할 것 등만을 권고하고 있다 10. 한의학에서 폐(肺)는 교장(嬌臟)이라고 하여 43, 오장(五臟) 중에서 가장 높은 표(表)에 해당하므로 외사(外邪)의 관문이 되어 쉽게 침입 당하고 외부와 직접 닿아있어 온도나 습도와 같은 외부 환경의 변화에 민감하므로 연약한 장기라고 하였다. 또한, ‘폐오조(肺惡燥)’ 43라고 하여 폐는 건조해 지면 쉽게 손상된다고 하였다. 이처럼 폐(肺)는 몸의 면역력을 담당하고 외부로부터 병사(病邪)의 침입을 방어하는 역할을 하여 쉽게 건조해지므로 44, 기관지를 윤택하게 하고(潤肺) 가래를 없애는 치료법이(化痰) 한의학에서 폐 손상을 막고 폐 기능을 개선시켜 주는 주된 치료방법으로 사용되어왔다. 윤폐화담(潤肺化痰)하는 대표적인 한약재로 길경, 맥문동, 행인, 과루인, 오미자 등이 있으며 45, 이를 통해 기관지의 염증을 제거하고 점막을 매끄럽게 하여 이물질의 자극에 과민반응을 일으키지 않도록 하였다. 기타 다양한 한약 제제들이 in vitro 및 in vivo 실험에서 미세먼지의 혈관 투과성 및 활성산소 감소효과, 폐 조직 손상 억제효과 등이 발표되었으며 46, 진해, 거담, 항균, 항염 작용을 통하여 미세먼지로부터 호흡기를 보호한다는 결과 47들이 발표되었다. 향후 위 한약제제들의 미세먼지 관련 임상연구가 진행되어야 할 필요가 있으며, 항 미세먼지 효과에 대한 한약제제 임상연구 설계 시 본 연구가 임상시험 기초자료로 활용되기를 바란다. 다만, 본 연구에서는 최근 심각성이 대두되고 있는 미세먼지의 영향에 초점을 맞추어 연구 동향을 파악하고자, ‘particulate matter’에 대한 MeSH Term만을 검색하여 분석하였기에 미세먼지를 포함하는 대기오염 관련 건강영향평가에 대한 문헌들까지 포함시키지는 못하였다. 미세먼지 관련 대규모 임상연구들은 대기오염의 범주에서 발표된 경우도 많아 향후 미세먼지의 호흡기 관련 영향에 대한 다양하고 전반적인 연구 동향의 파악을 위해서는 ‘particulate matter’의 상위어인 ‘air pollutants’ 등의 MeSH Term을 이용한 문헌 검색이 필요할 것으로 생각된다.
감사의 글
본 연구는 보건복지부 한의약선도기술개발사업의 지원(과제번호: HI15C006)과 2015년도 교육부의 재원으로 한국연구재단의 지원(과제번호: NRF -2015R1D1A1A01058852) 및 한국한의학연구원의 지원(과제코드: K17510)의 지원을 받아 수행되었음.
참고문헌
1. OECD. The economic consequences of outdoor air pollution 2016:6.
2. Pope CA 3rd, Dockery DW. Health effects of fine particulate air pollution:lines that connect. Journal of the air & waste management association 2006:56(6):709–42.   3. Lee MS. Government Policy Trends related to Particulate Matter. NEWS & INFORMATION FOR CHEMICAL ENGINEERS 35 No. 5 2017:
4. World Health Organization. Air pollution including WHO's 1999 guidelines for air pollution control Geneva: World Health Organization: 2000.
5. Begum BA, Biswas SK, Hopke PK. Source apportionment of air particulate matter by chemical mass balance (CMB) and comparison with positive matrix factorization (PMF) model. Aerosol and Air Quality Research 2007:7(4):446–68.  6. Air Quality Research Division. Study on the Composition of PM2.5 in the Yellow Sand and Fine Particle Incheon: National Institute of Environmental Research: 2008.
7. Seagrave J. Mechanisms and implications of air pollution particle associations with chemokines. Toxicology and applied pharmacology 2008:232(3):469–77.  8. Myong JP. Health effects of particulate matter. The Korean Journal of Medicine 2016:91(2):106–13. 9. Loomis D, Huang W, Chen G. The International Agency for Research on Cancer (IARC) evaluation of the carcinogenicity of outdoor air pollution:focus on China. Chinese journal of cancer 2014:33(4):189. 10. Kyung SY, Kim YS, Kim WJ, Park MS, Song JW, Yum H, et al. Guideline for the prevention and managementof particulate matter/Asian dust particleinduced adverse health effect on the patients withpulmonary diseases. Journal of the Korean Medical Association 2015:58(11):1060–9. 11. Donaldson K, Stone V, Borm PJ, Jimenez LA, Gilmour PS, Schins RP, et al. Oxidative stress and calcium signaling in the adverse effects of environmental particles (PM10). Free Radical Biology and Medicine 2003:34(11):1369–82. 12. Ministry of Health & Welfare. Health Impacts of Air Pollution in Korea 2016. Seoul: Korea:
13. Kleinman MT, Bailey RM, Whynot JD. Controlled exposure to a mixture of SO2, NO2, and particulate air pollutants:effects of human pulmonary function and respiratory symptoms. Archives of environmental health 1985:40(4):197–201. 14. Wang B, Peng Z, Zhang X, Xu Y, Wang H, Allen G, et al. Particulate matter, sulfur dioxide, and pulmonary function in never-smoking adults in Chongqing, China. International journal of occupational and environmental health :official journal of the International Commission on Occupational Health 1999:5(1):14–9. 15. Gong H Jr, Linn WS, Sioutas C, Terrell SL, Clark KW, Anderson KR, et al. Controlled exposures of healthy and asthmatic volunteers to concentrated ambient fine particles in Los Angeles. Inhal Toxicol 2003:15(4):305–25. 16. Slaughter JC, Lumley T, Sheppard L, Koenig JQ, Shapiro GG. Effects of ambient air pollution on symptom severity and medication use in children with asthma. Ann Allergy Asthma Immunol 2003:91(4):346–53. 17. Schildcrout JS, Sheppard L, Lumley T, Slaughter JC, Koenig JQ, Shapiro GG. Ambient air pollution and asthma exacerbations in children:an eight-city analysis. Am J Epidemiol 2006:164(6):505–17. 18. Bedada GB, Heinrich J, Götschi T, Downs SH, Forsberg B, Jarvis D, et al. Urban background particulate matter and allergic sensitization in adults of ECRHS II. International Journal of Hygiene and Environmental Health 2007:210(6):691–700. 19. Qian Z, Lin HM, Chinchilli VM, Lehman EB, Duan Y, Craig TJ, et al. Interaction of ambient air pollution with asthma medication on exhaled nitric oxide among asthmatics. Arch Environ Occup Health 2009:64(3):168–76. 20. Anderson HR, Ruggles R, Pandey KD, Kapetanakis V, Brunekreef B, Lai CK, et al. Ambient particulate pollution and the world-wide prevalence of asthma, rhinoconjunctivitis and eczema in children:Phase One of the International Study of Asthma and Allergies in Childhood (ISAAC). Occup Environ Med 2010:67(5):293–300. 21. Roy A, Hu W, Wei F, Korn L, Chapman RS, Zhang J. Ambient particulate matter and lung function growth in Chinese children. Epidemiology 2012:23(3):464–72. 22. Karottki DG, Spilak M, Frederiksen M, Gunnarsen L, Brauner EV, Kolarik B, et al. An indoor air filtration study in homes of elderly:cardiovascular and respiratory effects of exposure to particulate matter. Environmental health:a global access science source 2013:12:116. 23. Alexis NE, Huang YC, Rappold AG, Kehrl H, Devlin R, Peden DB. Patients with asthma demonstrate airway inflammation after exposure to concentrated ambient particulate matter. Am J Respir Crit Care Med 2014:190(2):235–7. 24. Guarnieri M, Diaz E, Pope D, Eisen EA, Mann J, Smith KR. Lung function in rural guatemalan women before and after a chimney stove intervention to reduce wood smoke exposure results from the randomized exposure study of pollution indoors and respiratory eff ects and chronic respiratory effects of early childhood exposure to respirable particulate matter study. Chest 2015:148(5):1184–92. 25. Kariisa M, Foraker R, Pennell M, Buckley T, Diaz P, Criner GJ, et al. Short- and long-term effects of ambient ozone and fine particulate matter on the respiratory health of chronic obstructive pulmonary disease subjects. Archives of environmental & occupational health 2015:70(1):56–62. 26. Zhou Y, Chen X, Zou W, Zhao D, Li X, Pu J, et al. Association between exposure to ambient particulate matter and chronic obstructive pulmonary disease:results from a cross-sectional study in China. Thorax (no pagination) 2016:2016:Date of Publication:December 16.
27. Meliton AY, Cho T, Hamanaka RB, Nigdelioglu R, Sun K, Budinger GS, et al. Short-term acute exposure of healthy humans to particulate matter induces differential gene expression in lung immune cells. American journal of respiratory and critical care medicine 2017:195:1. 28. Watanabe M, Noma H, Kurai J, Sano H, Hantan D, Ueki M, et al. A panel study of airborne particulate matter composition versus concentration:Potential for inflammatory response and impaired pulmonary function in children. Allergol Int 2017:66(1):52–8. 29. Holm SM, Balmes J, Gillette D, Hartin K, Seto E, Lindeman D, et al. Cooking behaviors are related to household particulate matter exposure in children with asthma in the urban East Bay Area of Northern California. PLoS One 2018:13(6):e0197199. 30. Pirozzi CS, Mendoza DL, Xu Y, Zhang Y, Scholand MB, Baughman RP. Short-Term Particulate Air Pollution Exposure is Associated with Increased Severity of Respiratory and Quality of Life Symptoms in Patients with Fibrotic Sarcoidosis. International journal of environmental research and public health 2018:15(6):1077. 31. Krishnan RM, Adar SD, Szpiro AA, Jorgensen NW, Van Hee VC, Barr RG, et al. Vascular responses to long- and short-term exposure to fine particulate matter:MESA Air (Multi-Ethnic Study of Atherosclerosis and Air Pollution). J Am Coll Cardiol 2012:60(21):2158–66. 32. Ristovski ZD, Miljevic B, Surawski NC, Morawska L, Fong KM, Goh F, et al. Respiratory health effects of diesel particulate matter. Respirology 2012:17(2):201–12. 33. Jang AS. Impact of particulate matter on health. Journal of the Korean Medical Association 2014:57(9):763–8. 34. Pope CA 3rd. Mortality effects of longer term exposures to fine particulate air pollution:review of recent epidemiological evidence. Inhalation toxicology 2007:19(sup1):33–8. 35. Air Quality Research Division. Study on the Composition of PM2.5 in the Yellow Sand and Fine Particle Incheon: National Institute of Environmental Research: 2008:
36. Choi YJ, Park JK, Jung WS. Synoptic Meteorological Classification of the Days on Which Asthma Deaths Occurred Due to High PM 10 Concentrations in Seoul. Journal of Environmental Science International 2017:26(2):159–72. 37. Seo JH, Ha EH, Lee BE, Park HS, Kim H, Hong YC, et al. The Effect of PM 10 on Respiratory-related Admission in Seoul. Journal of Korean Society for Atmospheric Environment 2006:22(5):564–73.
38. Kim OJ, Kim SJ, Kim H. Long-term exposure to fine particulate air pollution and mortality in a South Korean population-based cohort. The Korean Society of Environmental Toxicology 2017:2017(10):265.
39. Allen RW, Barn PK, Lanphear BP. Randomized controlled trials in environmental health research:unethical or underutilized? PLoS medicine 2015:12(1):e1001775. 40. Mann C. Observational research methods. Research design II:cohort, cross sectional, and case-control studies. Emergency medicine journal 2003:20(1):54–60. 41. Bruce N, Perez-Padilla R, Albalak R. The health effects of indoor air pollution exposure in developing countries. World Health Organization 2002:
42. Gong H Jr, Sioutas C, Linn WS. Controlled exposures of healthy and asthmatic volunteers to concentrated ambient particles in metropolitan Los Angeles. Res Rep Health Eff Inst 2003:118:1–36. discussion 7-47.
43. Ryu DG. DongUi-Physiology-GangUi Iksan: Wonkwang University Publisher: 1996. p. 215.
44. National Oriental Medicine College of Pumlonolgy. Pulmonology 2nd. Seoul: Nado: 2013. p. 8.
45. National Oriental Medicine College of Traditional herbal medicine. Traditional herbal medicine 2nd. Seoul: Jungeumsa: 2011. p. 497499, 513, 645, 683.
46. Lee W, Bae JS. Inhibitory effects of Kyung-Ok-Ko, traditional herbal prescription, on particulate matter-induced vascular barrier disruptive responses. International journal of environmental health research 2019:29(3):301–11. 47. Yang WK. Protective effect of GHX02 on particulate matter-induced lung injury. Daejeon University 2019:
|
|